Dr Oana Barnett (July, 2026)
| The NeuroAffective-CBT® Journal |
Abstract
Body Dysmorphic Disorder (BDD) is a debilitating psychological condition characterised by persistent preoccupation with perceived defects in physical appearance, often resulting in significant emotional distress, functional impairment, and repetitive safety behaviours. Although cognitive-behavioural therapy (CBT) remains the recommended psychological intervention for BDD, many individuals continue to experience recurrent symptoms despite previous therapeutic gains.
This case study introduces NeuroAffective-CBT (NA-CBT) through the treatment of “Sophie”, a woman in her fifties presenting with longstanding Body Dysmorphic Disorder, chronic shame, recurrent depression, insomnia, social withdrawal, and increasing psychological distress following menopause, occupational loss, and repeated cosmetic procedures. Rather than conceptualising these difficulties as isolated symptoms, NA-CBT formulated them as interacting manifestations of increased neuroaffective load, arising through the dynamic relationship between physiology, affect, cognition, autobiographical memory, and interpersonal experience.
Grounded within the cognitive behavioural tradition, NA-CBT integrates contemporary neuroscience, affective science, lifestyle medicine, and behavioural psychology while maintaining the collaborative, structured and evidence-informed principles that characterise CBT (Beck, 1976, 2021; Clark & Beck, 2010). Central to this formulation is the TED (Tired–Exercise–Diet) framework, alongside the Body–Brain–Affect Triangle, which together provide a practical model for understanding how physiological regulation influences affective processing, cognitive interpretation, and psychological flexibility (Mirea, 2023, 2025a, 2025b).
Treatment focused on reducing neuroaffective load, strengthening physiological regulation, facilitating NeuroAffective Narrative Reconsolidation, and supporting the gradual emergence of a more coherent and compassionate Integrated-Self. Throughout therapy, the therapist repeatedly returned to a simple but clinically significant question:
“What might be maintaining your neuroaffective load, and what might help reduce it?”
Rather than replacing established cognitive behavioural models of Body Dysmorphic Disorder, NA-CBT extends them by integrating affective neuroscience and physiological regulation into psychological formulation and intervention. This case study illustrates how an integrated neuroaffective perspective may enhance therapeutic understanding and contribute to the treatment of complex presentations characterised by chronic shame, self-criticism, and recurrent emotional distress.
Keywords: Body Dysmorphic Disorder; Cognitive Behavioural Therapy; NeuroAffective-CBT; Affect; Neuroscience; TED; Lifestyle Interventions; Integrated-Self.

Introduction
Body Dysmorphic Disorder (BDD) is characterised by persistent preoccupation with perceived defects in physical appearance that are either unobservable or appear slight to others (American Psychiatric Association, 2022). These concerns are typically accompanied by repetitive behaviours such as mirror checking, camouflage, reassurance seeking, appearance comparisons, and avoidance of social situations. The condition frequently results in profound impairment across occupational, interpersonal, and emotional domains and is associated with elevated rates of depression, anxiety, social isolation, and suicidality (Phillips, 2005; Phillips et al., 2010).
Cognitive Behavioural Therapy (CBT) remains the recommended psychological treatment for Body Dysmorphic Disorder, with substantial evidence supporting interventions targeting dysfunctional appearance beliefs, selective attention, avoidance, and safety behaviours (Veale, 2004; Veale & Neziroglu, 2010; Wilhelm et al., 2013). Nevertheless, many individuals continue to experience recurring symptoms following successful therapy, particularly when significant life transitions, physiological changes, or cumulative adversity increase emotional vulnerability.
These observations invite an important clinical question: Is recurrence always evidence that previous therapy has failed? Or might it reflect a profound change in the physiological and affective conditions within which previously acquired psychological skills are now expected to operate?
NeuroAffective-CBT (NA-CBT) emerged from this question. NA-CBT belongs firmly within the broad family of cognitive behavioural therapies. It retains the structured formulation, collaborative empiricism, behavioural experimentation, and evidence-informed practice that have long characterised CBT (Beck, 1976; Beck, 2021; Clark & Beck, 2010). What distinguishes NA-CBT is not a departure from cognitive behavioural principles, but a greater depth of integration. It draws together contemporary neuroscience, affective science, physiology, attachment, and behavioural psychology within a unified cognitive behavioural formulation (Damasio, 1999; LeDoux, 2015; Panksepp, 1998; Mirea, 2018).
Here, philosophy meets science. The body meets the mind.
Rather than conceptualising emotional distress as existing solely within cognition, NA-CBT understands psychological experience as emerging through continuous interactions between physiology, affective systems, cognitive interpretation, autobiographical memory, and interpersonal relationships. Mind and body are therefore not treated as separate domains requiring different explanatory models, but as components of a single, dynamically regulated neuroaffective system (Barrett, 2017; Friston, 2010; Siegel, 2012).
This perspective does not replace existing CBT models of Body Dysmorphic Disorder. Instead, it extends them by asking an additional question:
What neuroaffective conditions allow these cognitive and behavioural processes to become more or less dominant?
The following case study illustrates how this formulation informed the treatment of a woman with longstanding Body Dysmorphic Disorder whose psychological difficulties unfolded against a backdrop of increasing physiological, relational, and emotional burden.
Case Presentation

Sophie was a woman in her early fifties who self-referred for psychological therapy following a significant deterioration in her emotional wellbeing. She had previously completed a course of Cognitive Behavioural Therapy several years earlier, during which she developed a good understanding of the cognitive and behavioural processes maintaining her appearance concerns. She described this therapy positively and reported that it had enabled her to manage her symptoms effectively for a number of years.
However, by the time she returned to therapy, Sophie no longer felt able to access the psychological flexibility she had previously achieved.
Over the intervening years, she had undergone several cosmetic procedures in the hope of correcting perceived flaws in her appearance. Rather than reducing her distress, these interventions intensified her preoccupation, leaving her feeling increasingly disfigured and emotionally devastated. She subsequently became involved in prolonged legal proceedings against one of the practitioners, describing the experience as deeply invalidating and reinforcing her conviction that she had been permanently damaged.
Alongside these experiences, Sophie’s life had changed considerably. She was now navigating menopause, persistent insomnia, increasing fatigue, and declining physical energy. She had lost her employment and found it difficult to secure another position. The increasing reliance on online meetings following the COVID-19 pandemic intensified her appearance concerns, as seeing herself on camera throughout the working day became a persistent source of anxiety and self-monitoring. She frequently turned her camera off whenever possible and described feeling acutely self-conscious whenever she was visible on screen.
Socially, Sophie reported becoming increasingly isolated. Although married, she experienced growing emotional distance within her relationship and described feeling profoundly alone. Her family of origin remained abroad, limiting opportunities for support. She also spoke with increasing sadness about never having had children, describing this as a source of grief that had become more salient as she grew older.
Despite continuing to use many of the cognitive strategies she had learned previously, Sophie experienced overwhelming shame, chronic self-criticism, increasing avoidance, disrupted sleep, emotional exhaustion, and persistent beliefs that she was fundamentally defective. She no longer described herself as simply feeling unattractive.She described feeling broken.
From a conventional CBT perspective, these changes might reasonably be understood as an exacerbation of existing Body Dysmorphic Disorder following multiple adverse life events. From a NeuroAffective-CBT perspective, however, a different question emerged:
What had changed within Sophie’s neuroaffective system that made previously effective psychological strategies increasingly difficult to access?
Developmental Experiences and the Emergence of the Integrated-Self
Sophie’s appearance concerns did not emerge in isolation. As therapy progressed, it became increasingly apparent that her relationship with beauty, worth, and belonging had developed within a family environment in which physical appearance carried considerable emotional significance.
She described growing up with the implicit understanding that beauty was more than an aesthetic quality—it reflected character, value, and lovability. Family conversations frequently centred on appearance, and those considered physically attractive appeared to receive greater admiration, attention, and warmth. Beauty became quietly associated with being “a good person”, while ordinary appearance felt synonymous with being overlooked.
One figure came to symbolise this experience throughout Sophie’s childhood.
Her cousin was widely regarded within the family as exceptionally beautiful. Sophie recalled adults openly commenting on her cousin’s appearance with admiration and delight, describing her as special, elegant, and somehow different from everyone else. As a young girl, Sophie became convinced that if she could somehow become beautiful enough, she too might receive the same affection, recognition, and emotional closeness from her mother and older sister.
Although this belief was never explicitly stated, it gradually became woven into her understanding of herself and others.
Beauty became associated with safety.Acceptance became conditional. Worth became something that had to be earned.
From a NeuroAffective-CBT perspective, these experiences contributed to the development of Deeply Rooted Beliefs (DRBs) concerning identity, acceptance, and interpersonal value. Unlike automatic thoughts, DRBs are understood as emotionally organised assumptions that develop over repeated affective experiences and gradually shape how individuals interpret themselves, others, and the world (Beck, 1976; Mirea, 2018). These beliefs rarely operate at the level of deliberate reasoning. Instead, they become embedded within autobiographical memory, affective prediction, and patterns of physiological responding.
One childhood memory remained particularly vivid throughout therapy.
Sophie recalled accompanying her cousin into a shop during adolescence. Her cousin secretly stole an item before leaving the store. Moments later, the shop assistant stopped Sophie, accusing her of the theft. Despite Sophie’s repeated insistence that she had done nothing wrong, the accusation continued. What remained most emotionally significant was not the theft itself, but the explanation she believed lay behind the accusation.
She recalled the shop assistant commenting that her cousin “looked too beautiful” to have stolen anything, whereas Sophie, with her darker features, “looked like the sort of person who would.” Whether these words were remembered verbatim or reconstructed over time became less important than the emotional meaning they continued to hold.
For Sophie, the experience crystallised a painful conclusion:
“People see something bad in me before they know me.”
The memory became one of the earliest examples of shame becoming organised not around behaviour, but around identity.
Many years later, this image continued to intrude unexpectedly. It frequently emerged before social situations, during work meetings, while shopping, and whenever Sophie felt herself being observed. Although intellectually she recognised the event belonged to the past, emotionally it continued to feel immediate. Her body responded as though the judgement were happening again in the present.
From a NeuroAffective-CBT perspective, such memories are understood not simply as autobiographical recollections but as emotionally encoded experiences that continue to influence present-day prediction and affective regulation (Lane et al., 2015; Brewin, 2014). Rather than remaining historical events, they become living templates through which new interpersonal experiences are interpreted.
Importantly, therapy did not conceptualise these experiences as evidence of a permanently fragmented self.
Instead, NA-CBT assumes that beneath layers of shame, fear, self-protection, and defensive adaptation lies an Integrated-Self, a coherent and compassionate sense of identity that has become increasingly difficult to access under conditions of sustained neuroaffective load (Mirea, 2018).
The therapeutic task therefore shifts. Rather than asking how the fragmented self can be repaired, NA-CBT asks:
What conditions might allow the Integrated Self to emerge more consistently?
This subtle change in formulation proved clinically important. It invited both therapist and client to become curious about the conditions supporting psychological integration, rather than focusing exclusively on pathology or symptom reduction.

Pause for Curiosity
Perhaps the most important question was no longer:
“Why does Sophie continue to experience Body Dysmorphic Disorder?”
Instead, therapy repeatedly returned to a different question:
“What might be maintaining Sophie’s neuroaffective load, and what might help reduce it?”
This question became a recurring anchor throughout therapy.
Rather than assuming that distress reflected psychological weakness or therapeutic failure, it invited curiosity about the interaction between physiology, affect, cognition, memory, relationships, and the broader context in which emotional regulation was taking place.
Within NeuroAffective-CBT, curiosity is not simply a therapeutic attitude.
It is a clinical intervention.

Neuroaffective Formulation
The developmental formulation helped explain why Sophie’s appearance concerns had become so emotionally significant. The next therapeutic question was equally important:
Why had these difficulties intensified now, after several years of relative stability?
Although Sophie retained many of the cognitive insights she had developed during her previous course of CBT, she increasingly described feeling unable to access them during periods of emotional distress. She understood that her thoughts were often biased, recognised many of her appearance-related safety behaviours, and could frequently identify alternative interpretations. Yet these skills no longer seemed sufficient to regulate the intensity of her emotional experience.
Rather than viewing this as evidence that therapy had failed, NA-CBT approached it as evidence that the neuroaffective conditions within which these cognitive skills operated had fundamentally changed.
Over recent years Sophie had experienced the cumulative impact of persistent insomnia, menopausal transition, occupational loss, increasing social isolation, repeated cosmetic procedures, prolonged legal proceedings, reduced physical activity, and the gradual erosion of interpersonal support. Each experience contributed not simply to “stress,” but to an increasing burden on the systems responsible for physiological regulation, emotional processing, and cognitive flexibility.
Within NeuroAffective-CBT, this accumulation is conceptualised as neuroaffective load (Mirea, 2018).
Neuroaffective load refers to the cumulative demands placed upon the integrated body-brain system through ongoing physiological dysregulation, affective activation, interpersonal adversity, cognitive burden, and environmental pressures. Unlike the broader concept of stress, neuroaffective load emphasises the dynamic interaction between bodily regulation and psychological functioning. It recognises that emotional suffering often emerges not from a single precipitating event but from the gradual accumulation of multiple interacting influences that reduce the nervous system’s capacity for flexible adaptation.
This distinction proved clinically meaningful.
When Sophie was invited to consider her difficulties through the lens of neuroaffective load, her experience began to make sense in a different way. Rather than concluding that she had “gone backwards” or that she had somehow lost the benefits of her previous therapy, she became increasingly able to understand why familiar psychological strategies were becoming harder to access.
Her brain had not forgotten what she had learned. It was working under very different physiological and affective conditions. This understanding became one of the most compassionate moments within therapy. Rather than asking,
“Why can’t I cope anymore?”
Sophie gradually found herself asking,
“What has happened to my system that makes coping so much harder?”
The question itself represented an important therapeutic shift.

Pause for Curiosity
Perhaps psychological resilience is not simply a characteristic that people possess.
Perhaps it is an emergent property of a nervous system that has sufficient physiological and emotional capacity to remain flexible.
If so, therapy may need to become curious not only about thoughts and behaviours, but about the conditions that either increase or reduce neuroaffective load.

This broader perspective also complements established cognitive behavioural models of Body Dysmorphic Disorder, which emphasise dysfunctional appearance beliefs, selective attention, mirror checking, reassurance seeking, avoidance, and safety behaviours in maintaining distress (Veale, 2004; Veale & Neziroglu, 2010; Phillips, 2005; Wilhelm et al., 2013). Rather than replacing these well-established formulations, NA-CBT seeks to extend them by incorporating physiological regulation, affective neuroscience, and predictive brain processes as interacting influences on these cognitive and behavioural maintenance cycles.
In doing so, the formulation broadens the therapeutic focus. The question is no longer solely,
“What thoughts maintain the problem?” but also,
“What neuroaffective conditions make these thoughts feel so compelling?”
Mind, Body, and the Foundations of Change
Many people enter psychotherapy believing that their emotional difficulties exist primarily “in the mind.” From a NeuroAffective-CBT perspective, this understanding is incomplete.
Mind and body form a single regulatory system. Thoughts influence physiology. Physiology influences affect. Affect shapes interpretation. Interpretation influences subsequent physiological responding.
Each component continuously influences the others within an ongoing cycle of prediction and regulation (Barrett, 2017; Damasio, 1999; Friston, 2010).
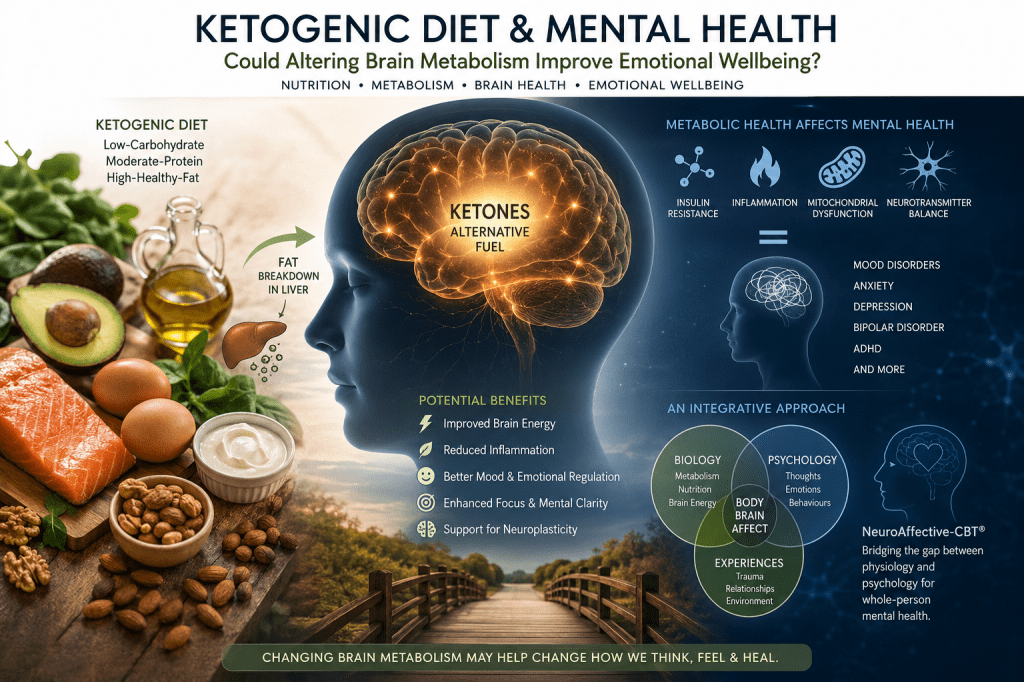
For this reason, NA-CBT integrates TED (Tired–Exercise–Diet) as a core stabilisation framework within psychotherapy (Mirea, 2023, 2025a, 2025b).
TED is not presented as a lifestyle programme or a substitute for psychological therapy. Nor does the NA-CBT therapist assume the role of a dietitian, physician, physiotherapist, or exercise professional. Instead, TED provides a psychologically informed framework through which clinicians explore how sleep, movement, nutrition, energy regulation, and everyday physiological functioning influence emotional experience and psychological flexibility. Where appropriate, clients are supported to access other healthcare professionals with specialist expertise in these areas.
This distinction is important. NeuroAffective-CBT is not practising medicine, nor is it reducing psychotherapy to lifestyle advice. Rather, it recognises that psychotherapy takes place within a living nervous system. Understanding how physiological regulation interacts with emotional processing enables the therapist to formulate distress more comprehensively and to collaborate with clients in reducing factors that unnecessarily increase neuroaffective load.
For Sophie, this became an essential component of therapy. Rather than viewing chronic fatigue, menopausal changes, insomnia, reduced physical activity, and nutritional habits as separate concerns to be addressed elsewhere, they became integrated into the psychological formulation. Together they provided important clues regarding the conditions under which shame intensified, emotional flexibility diminished, and appearance concerns became increasingly dominant.
Consequently, therapy frequently returned to one practical question:
What might be maintaining your neuroaffective load, and what might help reduce it?
This question gradually became the organising principle of treatment.
Rather than functioning as a checklist, it encouraged collaborative curiosity. It also translated naturally into collaborative goal setting. Together, therapist and Sophie began distinguishing between behaviours that appeared to maintain neuroaffective load and those that helped reduce neuroaffective load.
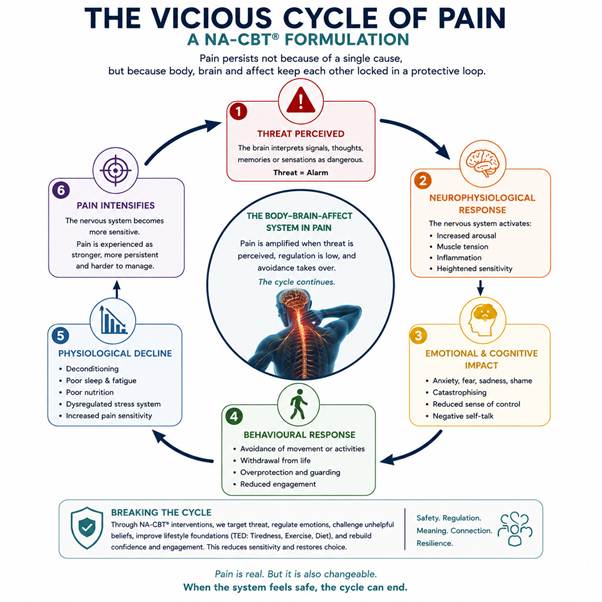
Visually, this was represented using two interconnected formulations.
The first resembled the familiar CBT vicious cycle, illustrating how poor sleep, inactivity, shame, social withdrawal, mirror checking, self-criticism, and avoidance interacted to perpetuate neuroaffective load.
Alongside this, therapist and client gradually constructed what Sophie came to call her virtuous flower. Each petal represented a small but meaningful influence that helped restore regulation: improved sleep routines, gentle movement, stretching, regular meals, meaningful social connection, compassionate self-reflection, behavioural experiments, and valued activity. No single intervention transformed her wellbeing. Collectively, however, they gradually altered the physiological and emotional context within which change became possible.
This visual distinction proved particularly helpful because it extended familiar CBT formulation without replacing it. Sophie immediately recognised its structure while simultaneously appreciating that the therapeutic focus had broadened beyond cognition alone.
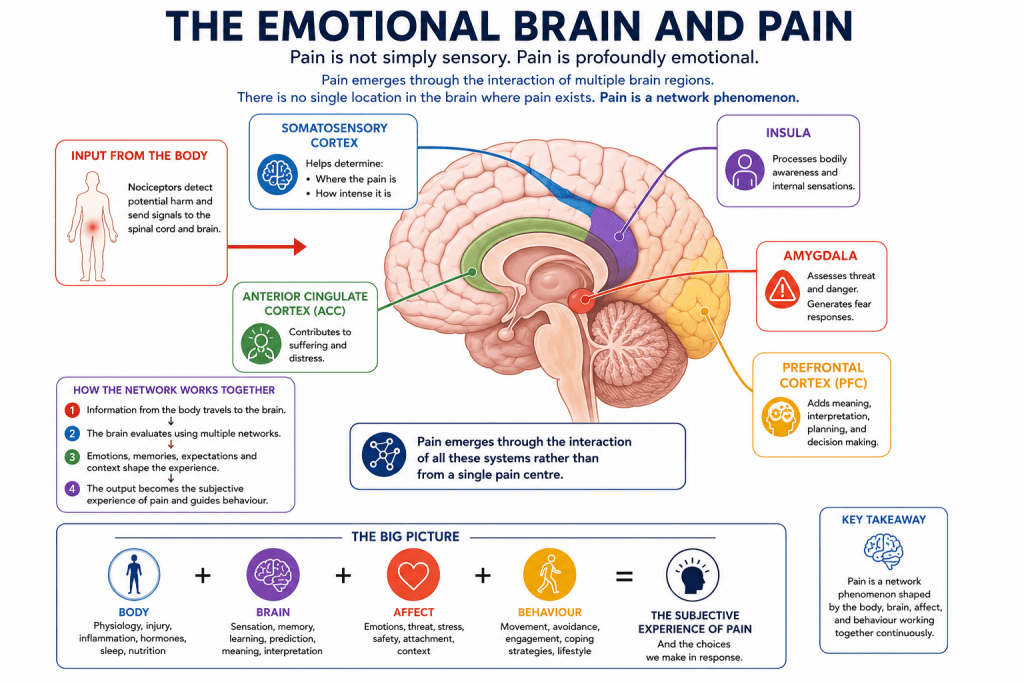
The Body–Brain–Affect Triangle

Central to NeuroAffective-CBT is the Body–Brain–Affect Triangle, a formulation that conceptualises psychological functioning as a continuously interacting regulatory system rather than a sequence of isolated psychological events. Drawing upon affective neuroscience, predictive processing, and embodied cognition, the triangle proposes that physiological regulation, predictive brain processes, and primary affective systems are engaged in a constant reciprocal dialogue (Panksepp, 1998; Damasio, 1999; Friston, 2010; Barrett, 2017; LeDoux, 2015).
Within this model, none of the three components operates independently. A change within one corner of the triangle inevitably influences the others, often before conscious awareness emerges.
Body (Physiology)
The body provides the biological context within which psychological experience unfolds. Sleep, movement, nutrition, hormonal functioning, autonomic regulation, metabolic stability, chronic pain, illness, and fatigue all influence the nervous system’s capacity to regulate emotional experience.
From this perspective, physiology is not simply a background variable. It is an active participant in emotional life.
When physiological regulation becomes compromised through chronic sleep disruption, hormonal transition, nutritional imbalance, prolonged inactivity, or persistent stress, the nervous system becomes increasingly sensitive to perceived threat. Emotional reactions occur more readily, remain active for longer, and become progressively more difficult to regulate.
Brain (Prediction and Interpretation)
Within NeuroAffective-CBT, the brain is understood primarily as a predictive organ whose central evolutionary function is protection rather than objective perception (Friston, 2010; Barrett, 2017).
Long before conscious reasoning begins, the brain is continuously asking:
“Am I safe?”
“What is about to happen?”
“What should I prepare for?”
“How bad could this become?”
These predictions are shaped not only by conscious beliefs and interpretations but also by bodily sensations, previous emotional learning, autobiographical memory, attachment experiences, and current physiological state.
Consequently, individuals rarely respond to the world exactly as it is.
They respond to the brain’s best prediction of what is about to happen.
When physiology becomes dysregulated, these predictive systems become increasingly threat-sensitive. Neutral situations are more easily interpreted as dangerous. Ambiguous facial expressions appear rejecting. Minor imperfections become overwhelming evidence of failure. Shame becomes more readily activated and more difficult to regulate.
Affect (Primary Emotional Systems)
Affect represents the fast, evolutionarily conserved emotional systems that organise survival long before reflective thinking becomes possible (Panksepp, 1998; LeDoux, 2015).
Fear. Shame. Disgust. Anger. Relief.
These emotional systems rapidly orient attention towards information relevant to survival and social belonging. Only afterwards does cognition begin constructing explanations for what has already been felt.
Within NeuroAffective-CBT, cognition therefore remains critically important, but it is understood as the meaning-making layer built upon ongoing physiological and affective activity. Emotions are not simply generated by thoughts, nor are thoughts merely reactions to emotions. Each continuously shapes the other within an integrated regulatory system.
Differentiating Affect from Interpretation
One of the central therapeutic aims of NeuroAffective-CBT is helping clients distinguish between raw affect and interpretation.
Raw affect refers to the body’s immediate emotional signal—fear, shame, sadness, anger, or relief—generated rapidly in response to internal or external cues.
Interpretation refers to the meaning subsequently assigned to those emotional signals through prediction, memory, beliefs, and conscious reflection (Barrett, 2017; Damasio, 1999).
When affect and interpretation become fused, emotional experiences begin to feel absolute.
“I feel ashamed” gradually becomes “I am shameful.”
“I feel afraid” becomes “I am unsafe.”
“I feel unattractive” becomes “I am fundamentally defective.”
Helping Sophie recognise this distinction became transformative. She gradually learned that the intensity of her emotional experience did not necessarily provide accurate information about objective reality. Instead, emotions increasingly became understood as important signals requiring curiosity rather than unquestioning acceptance.
Therapy repeatedly slowed these moments by returning to a more fundamental question:
What is your body signalling right now?
followed by..
Is your brain interpreting that signal in a way that accurately reflects the present?
These questions gradually interrupted the automatic fusion of affect and identity that had characterised Sophie’s experience for many years.
Therapeutic Process
The therapeutic process unfolded over approximately twelve months through weekly outpatient sessions. Although therapy retained the collaborative structure characteristic of Cognitive Behavioural Therapy, the emphasis gradually shifted from challenging isolated cognitions towards understanding the broader neuroaffective conditions within which those cognitions emerged.
From the outset, formulation became a collaborative process of curiosity rather than explanation. Rather than seeking a single underlying cause for Sophie’s distress, therapy explored how developmental experiences, current relationships, physiological regulation, affective responses, autobiographical memory, and behavioural patterns interacted to maintain her psychological difficulties.
Sophie’s previous CBT had equipped her with valuable cognitive skills. These were not discarded or replaced. Instead, they were revisited within a broader formulation that recognised why accessing these skills had become increasingly difficult under conditions of elevated neuroaffective load.
Behavioural experiments therefore remained central to therapy, but their purpose subtly expanded.
Rather than asking only, “What evidence supports this belief?” therapy increasingly asked,
“What happens to your emotional experience when your nervous system is more regulated?”
And “How does reducing neuroaffective load influence your ability to think differently?”
This shift was particularly evident when addressing mirror checking, avoidance, and appearance-focused behaviours.
Previously, behavioural experiments had focused primarily on testing catastrophic beliefs concerning Sophie’s appearance.
Within NA-CBT, these experiments continued, but they were carefully timed to coincide with periods of improved physiological regulation whenever possible. Sessions frequently explored the relationship between sleep quality, physical activity, emotional intensity, and the outcomes of behavioural experiments.
Over time, Sophie herself began noticing an important pattern. On days following adequate sleep, regular movement, and greater physiological stability, behavioural experiments felt challenging but manageable. Following several nights of poor sleep or heightened emotional exhaustion, identical experiments often felt overwhelming. This observation reinforced one of the central propositions of NA-CBT:
Psychological flexibility is not determined solely by cognitive skill. It is profoundly influenced by the physiological and affective conditions within which those skills are required.

Pause for Curiosity
Perhaps therapy becomes most effective not when clients think differently first…
…but when the conditions exist that allow different thinking to become possible.

NeuroAffective Narrative Reconsolidation (NNR)
As Sophie’s neuroaffective load gradually reduced, a notable shift began to emerge within therapy. She did not simply experience fewer distressing thoughts or engage in fewer appearance-related safety behaviours. Rather, she began relating to herself differently.
This change was subtle at first. Memories that had previously felt emotionally overwhelming became easier to approach. Shame remained present but no longer felt all-encompassing. Situations that once automatically confirmed long-held beliefs of defectiveness began to acquire alternative meanings.
Importantly, these changes did not arise through repeated attempts to replace “irrational thoughts” with more rational alternatives alone. Instead, they appeared to emerge as Sophie’s nervous system became increasingly able to tolerate emotional experience without immediately defaulting to threat-based prediction.
One memory proved particularly significant.
Throughout therapy, Sophie repeatedly returned to the childhood incident in which she had been accused of stealing after her cousin concealed an item in a shop. For many years she had experienced this memory not simply as an unfortunate childhood event but as compelling evidence that other people instinctively saw her as fundamentally bad, suspicious, or unworthy.
Earlier in life she had attempted to challenge this conclusion intellectually. She understood that the accusation had been unfair and recognised that many people would interpret the situation differently.
Yet this cognitive understanding had done little to alter the emotional meaning carried by the memory. Within NA-CBT, the therapeutic task therefore became different.
Rather than attempting to dispute the factual accuracy of the event, therapy sought to understand how its emotional significance had become organised within Sophie’s broader neuroaffective system.
The memory was no longer viewed in isolation. It became connected to a much wider developmental narrative. Repeated experiences in which beauty appeared to determine acceptance. The gradual belief that being attractive was necessary to deserve love. The experience of becoming increasingly invisible within important relationships. The emotional impact of repeated cosmetic procedures that left her feeling more flawed rather than less. The grief associated with childlessness. The loneliness she experienced within her marriage. The loss of work and identity. The exhaustion associated with chronic insomnia and menopause.
Together, these experiences formed an interconnected autobiographical narrative organised around a central expectation: “There is something fundamentally wrong with me.”
Within NeuroAffective-CBT, this process is conceptualised as NeuroAffective Narrative Reconsolidation (NNR).
NNR describes the gradual revision of emotionally organised autobiographical narratives through repeated experiences of physiological regulation, emotional safety, cognitive flexibility, and corrective interpersonal experience. Rather than focusing solely on changing individual beliefs, NNR seeks to reorganise the broader narrative structures through which people understand themselves, others, and the world. This understanding is consistent with contemporary theories of memory reconsolidation and emotional learning, which suggest that previously established emotional meanings remain open to revision when reactivated under conditions that permit new learning (Lane et al., 2015; Brewin, 2014; Arntz, 2012).
For Sophie, this process unfolded gradually rather than dramatically.
There was no single transformative session. Instead, countless small moments accumulated. She noticed herself remaining on camera for slightly longer during online meetings. She accepted invitations that she would previously have declined. She looked in the mirror without immediately searching for defects. She found herself walking outside without feeling compelled to hide behind sunglasses or heavy make-up. Most importantly, she became increasingly able to experience shame without allowing it to define her identity.
One session illustrated this particularly clearly. While discussing the childhood shop incident, Sophie paused and quietly said,
“I think I spent most of my life trying to prove that they were wrong.” ..“Maybe I don’t need to prove anything anymore.”
This moment was not interpreted as the disappearance of shame. Nor did it represent the complete resolution of Body Dysmorphic Disorder. Instead, it reflected a profound reorganisation of meaning. The memory remained but its emotional authority had changed. Rather than functioning as unquestioned evidence of personal defectiveness, it became recognised as one painful chapter within a much larger life story.
From that point onwards, the memory could be held with compassion rather than certainty.
The Emergence of the Integrated-Self
Throughout therapy, the central therapeutic aim was never to eliminate unwanted emotions or construct an idealised version of the self.
Instead, NA-CBT sought to create the neuroaffective conditions in which Sophie’s Integrated-Self could emerge more consistently.
The Integrated Self does not represent perfection, permanent happiness, or the absence of vulnerability.
Rather, it reflects an increasingly coherent experience of identity in which physiology, affect, cognition, behaviour, autobiographical memory, and interpersonal experience become more harmoniously aligned.
Within this state, emotional experiences remain meaningful without becoming overwhelming.
Thoughts remain influential without becoming absolute. The body becomes a source of information rather than threat. Relationships become opportunities for connection rather than continual evaluation. Most importantly, identity becomes less organised around protection and more organised around authenticity.
This distinction proved fundamental. Early in therapy, Sophie experienced herself almost entirely through the lens of shame. Later, she increasingly recognised shame as one emotional experience among many. The difference was profound as she no longer experienced what she felt as who she was. Instead, emotions became experiences that could be observed, understood, and responded to with increasing flexibility.
As the Integrated-Self became more accessible, behavioural change emerged naturally rather than through constant effort. Mirror checking reduced, avoidance diminished and social engagement gradually increased. Self-care became motivated less by fear of judgement and more by genuine compassion for herself. Perhaps most significantly, therapy no longer revolved around repairing a defective person.
Instead, it focused on creating the biological, psychological, and relational conditions that allowed an already existing, though previously obscured, sense of self to become increasingly available.

Pause for Curiosity
Perhaps psychological change is not always about becoming someone new.
Perhaps it is about reducing the neuroaffective conditions that prevent people from becoming who they have always had the capacity to be.

Discussion
Sophie’s therapeutic journey illustrates one of the central propositions of NeuroAffective-CBT: the recurrence of psychological symptoms does not necessarily indicate that previous therapy has been unsuccessful. Rather, it may reflect profound changes in the neuroaffective context within which previously acquired psychological skills are now expected to operate.
Although Sophie retained many of the cognitive insights developed during her previous course of CBT, years of accumulating physiological, relational, occupational, and emotional adversity had fundamentally altered the conditions under which these skills were required. Menopause, persistent insomnia, occupational loss, social isolation, repeated cosmetic procedures, prolonged litigation, and unresolved grief collectively increased her neuroaffective load, reducing psychological flexibility despite preserved cognitive understanding.
Rather than conceptualising this deterioration as therapeutic failure, NA-CBT understood it as evidence that cognition does not operate independently of physiology and affect. Cognitive restructuring, behavioural experiments, and exposure remain essential components of evidence-based treatment (Beck, 1976, 2021; Clark & Beck, 2010). However, the effectiveness of these interventions may be influenced by the physiological and affective state within which they occur.
This broader formulation complements established cognitive behavioural models of Body Dysmorphic Disorder, which emphasise dysfunctional appearance beliefs, selective attention, mirror checking, avoidance, reassurance seeking, and safety behaviours in maintaining distress (Veale, 2004; Veale & Neziroglu, 2010; Phillips, 2005; Wilhelm et al., 2013). Rather than replacing these well-established models, NeuroAffective-CBT seeks to extend them by incorporating physiological regulation, predictive processing, and affective neuroscience into psychological formulation.
From this perspective, body dysmorphic symptoms are understood not only as products of maladaptive cognition and behaviour but also as emerging within an integrated body-brain system continuously attempting to predict, interpret, and respond to potential threat (Friston, 2010; Barrett, 2017). The brain’s primary evolutionary task is not objective reasoning but anticipation in the service of protection. Consequently, alterations in physiological regulation may significantly influence the intensity, persistence, and credibility of appearance-related beliefs.
Central to this formulation is the concept of neuroaffective load (Mirea, 2018). Unlike broader notions of stress, neuroaffective load refers to the cumulative interaction between physiological dysregulation, affective activation, cognitive burden, interpersonal adversity, and environmental demands. Sophie’s presentation illustrated how multiple seemingly independent difficulties gradually converged to create conditions in which shame, self-criticism, and avoidance became increasingly dominant.
The introduction of the TED (Tired–Exercise–Diet) framework provided a practical means of addressing these physiological influences within psychotherapy (Mirea, 2023, 2025a, 2025b). Importantly, TED is not intended to replace specialist medical, nutritional, or exercise interventions. Rather, it offers psychologists a psychologically informed framework through which physiological regulation becomes part of collaborative formulation. Where clinically appropriate, clients may be supported to access relevant healthcare professionals while psychotherapy continues to address the emotional and cognitive implications of physiological dysregulation.
One of the distinguishing features of NA-CBT is its explicit rejection of a traditional mind-body dichotomy. Rather than viewing biological and psychological processes as separate domains, NA-CBT conceptualises emotional experience as emerging through continuous interactions between physiology, affect, cognition, autobiographical memory, and interpersonal relationships (Damasio, 1999; Barrett, 2017; Siegel, 2012). The Body-Brain-Affect Triangle offers one way of organising these interactions clinically, helping therapists and clients appreciate how changes in one component inevitably influence the others.
Another important contribution concerns the distinction between affect and interpretation. Throughout therapy, Sophie gradually learned to differentiate immediate emotional signals from the meanings subsequently assigned to them. This distinction allowed shame to become an emotional experience rather than a fixed identity. Increasingly, she recognised that intense emotional reactions were not necessarily accurate reflections of present reality but understandable responses generated within a nervous system organised around protection rather than objective perception (LeDoux, 2015; Panksepp, 1998).
These developments created the conditions for NeuroAffective Narrative Reconsolidation. Rather than focusing exclusively on modifying individual cognitions, therapy facilitated the gradual reorganisation of emotionally significant autobiographical narratives. Memories that had long functioned as unquestioned evidence of personal defectiveness became integrated into a broader, more compassionate life story. This process aligns conceptually with contemporary understandings of memory reconsolidation and emotional learning, suggesting that autobiographical narratives remain open to revision when reactivated under conditions of sufficient emotional safety and physiological regulation (Lane et al., 2015; Brewin, 2014; Arntz, 2012).
Perhaps most importantly, the therapeutic goal extended beyond symptom reduction. While reductions in appearance preoccupation, avoidance, and self-criticism were clinically meaningful, they were understood as consequences of a broader developmental process rather than endpoints in themselves. The overarching aim became the emergence of an Integrated-Self, a coherent experience of identity in which physiology, affect, cognition, autobiographical memory, behaviour, and relationships become increasingly aligned (Mirea, 2018).
Throughout treatment, one recurring question appeared to organise both formulation and intervention:
What might be maintaining your neuroaffective load, and what might help reduce it?
Although deceptively simple, this question repeatedly redirected attention away from self-blame and towards collaborative curiosity. It also proved highly transportable across therapeutic goals, helping distinguish behaviours that maintained neuroaffective load from those that gradually reduced it. In Sophie’s therapy, this distinction was represented visually through a traditional CBT vicious cycle alongside a complementary “virtuous flower”, illustrating the multiple pathways through which physiological regulation, valued action, behavioural flexibility, and compassionate self-care gradually supported psychological recovery.
Limitations
As a single case study, the present report cannot determine the efficacy of NeuroAffective-CBT or establish causal relationships between specific interventions and clinical outcomes. Improvements observed throughout therapy likely reflected the combined influence of multiple therapeutic, interpersonal, and contextual factors.
Accordingly, the present case should be viewed as an illustration of clinical formulation rather than evidence of treatment superiority. Future research should evaluate NA-CBT across a range of clinical presentations using controlled methodologies, examining both symptom outcomes and broader indicators of physiological regulation, emotional flexibility, identity integration, and quality of life.
Future Directions
Future developments within NeuroAffective-CBT should focus on systematic empirical evaluation of the model across anxiety disorders, obsessive-compulsive and related disorders, mood disorders, trauma-related presentations, and personality difficulties. In particular, research exploring interactions between physiological regulation, affective processing, and cognitive flexibility may further clarify the mechanisms through which neuroaffective load influences psychological functioning. Finally, future publications may expand the present work by exploring the theoretical foundations of NA-CBT in greater depth, alongside additional clinical illustrations across diverse diagnostic presentations.
Conclusion
This case study has presented NeuroAffective-CBT (NA-CBT) through the treatment of a woman with longstanding Body Dysmorphic Disorder whose difficulties evolved within the context of cumulative physiological, developmental, relational, and emotional adversity. Rather than conceptualising symptom recurrence as evidence of therapeutic failure, NA-CBT proposed that previously acquired psychological skills had become increasingly difficult to access because the neuroaffective conditions supporting their effective use had fundamentally changed.
Throughout therapy, formulation extended beyond cognition alone to consider the continuous interaction between physiology, affect, predictive brain processes, autobiographical memory, behaviour, and interpersonal experience. Concepts such as neuroaffective load, the TED (Tired–Exercise–Diet) framework, the Body–Brain–Affect Triangle, and NeuroAffective Narrative Reconsolidation provided an integrated framework through which Sophie’s presentation became increasingly understandable and clinically meaningful.
Importantly, NA-CBT does not seek to replace established cognitive behavioural models. Instead, it builds upon the considerable strengths of contemporary CBT by incorporating developments from affective neuroscience, predictive processing, embodied cognition, attachment theory, and lifestyle medicine into psychological formulation and intervention (Beck, 2021; Barrett, 2017; Friston, 2010). In doing so, it offers clinicians an expanded framework for understanding how physiological regulation, emotional processing, and cognitive flexibility continuously influence one another.
Perhaps the most significant shift within therapy concerned its ultimate aim.
Rather than striving simply to reduce symptoms, challenge distorted cognitions, or eliminate distress, treatment sought to create the biological, psychological, and relational conditions in which Sophie’s Integrated-Self could emerge more consistently. As neuroaffective load gradually reduced, shame became less defining, autobiographical memories acquired new meaning, behavioural flexibility increased, and compassion gradually replaced self-protection as the organising principle of her relationship with herself.
At its heart, NeuroAffective-CBT invites clinicians to become curious. Curious about the relationship between body and mind. Curious about the interaction between physiology and cognition. Curious about how affect shapes prediction before conscious thought has emerged. Curious about the stories people carry about themselves and the neuroaffective conditions that allow those stories to evolve.
Clinical Reflections
This case illustrates how broadening formulation beyond cognition alone may enrich clinical understanding without abandoning the principles of Cognitive Behavioural Therapy. The concepts presented within NA-CBT are intended to complement—not replace—existing evidence-based CBT models. Throughout treatment, curiosity functioned not merely as a therapeutic attitude but as an active clinical intervention, encouraging therapist and client to explore how physiology, affect, cognition, memory, and relationships continuously interacted.
For practising clinicians, the recurring question— What might be maintaining neuroaffective load, and what might help reduce it? —may provide a simple yet clinically useful organising principle that readily translates into collaborative formulation, treatment planning, behavioural goals, and relapse prevention.

Disclaimer
This case study is intended solely for educational and professional discussion purposes. It does not constitute clinical guidance, diagnosis, or treatment recommendations. Therapeutic approaches described should be implemented only by appropriately trained professionals within their scope of competence and adapted to the individual needs of each client. Readers are encouraged to consult relevant clinical guidelines, current evidence, and professional supervision when applying the concepts presented within this paper.
The image used in this article is an illustrative image only. This image is AI-generated and does not depict the actual client. It has been created solely to reflect the themes of this anonymised case study.
Ethics and Anonymisation Statement
All identifying client information has been altered to protect anonymity. The case has been substantially anonymised, and contextual details have been modified where necessary to minimise the possibility of identification while preserving the clinical relevance of the formulation. Informed consent was obtained for the use of anonymised clinical material for educational and dissemination purposes.

References
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.; DSM-5-TR). American Psychiatric Association.
Arntz, A. (2012). Imagery rescripting as a therapeutic technique: Review of clinical trials, basic studies, and research agenda. Journal of Experimental Psychopathology, 3(2), 189–208. https://doi.org/10.5127/jep.024211
Barrett, L. F. (2017). How emotions are made: The secret life of the brain. Houghton Mifflin Harcourt.
Barrett, L. F., & Simmons, W. K. (2015). Interoceptive predictions in the brain. Nature Reviews Neuroscience, 16(7), 419–429. https://doi.org/10.1038/nrn3950
Beck, A. T. (1976). Cognitive therapy and the emotional disorders. International Universities Press.
Beck, J. S. (2021). Cognitive behavior therapy: Basics and beyond (3rd ed.). Guilford Press.
Brewin, C. R. (2014). Episodic memory, perceptual memory, and their interaction: Foundations for a theory of posttraumatic stress disorder. Psychological Bulletin, 140(1), 69–97. https://doi.org/10.1037/a0033722
Clark, A. (2013). Whatever next? Predictive brains, situated agents, and the future of cognitive science. Behavioral and Brain Sciences, 36(3), 181–204. https://doi.org/10.1017/S0140525X12000477
Clark, D. A., & Beck, A. T. (2010). Cognitive therapy of anxiety disorders: Science and practice. Guilford Press.
Damasio, A. (1999). The feeling of what happens: Body and emotion in the making of consciousness. Harcourt Brace.
Elsey, J. W. B., Van Ast, V. A., & Kindt, M. (2018). Human memory reconsolidation: A guiding framework and critical review. Neuroscience & Biobehavioral Reviews, 89, 1–19. https://doi.org/10.1016/j.neubiorev.2018.03.008
Firth, J., Solmi, M., Wootton, R. E., et al. (2020). A meta-review of lifestyle psychiatry: The role of exercise, smoking, diet and sleep in the prevention and treatment of mental disorders. World Psychiatry, 19(3), 360–380. https://doi.org/10.1002/wps.20773
Friston, K. (2010). The free-energy principle: A unified brain theory? Nature Reviews Neuroscience, 11(2), 127–138. https://doi.org/10.1038/nrn2787
Hayes, S. C., Hofmann, S. G., & Ciarrochi, J. (2022). A process-based approach to psychological diagnosis and treatment. Current Directions in Psychological Science, 31(4), 343–350. https://doi.org/10.1177/09637214221089356
Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (2012). Acceptance and commitment therapy: The process and practice of mindful change (2nd ed.). Guilford Press.
Hofmann, S. G., & Hayes, S. C. (2019). The future of intervention science: Process-based therapy. Clinical Psychological Science, 7(1), 37–50. https://doi.org/10.1177/2167702618772296
Hohwy, J. (2020). New directions in predictive processing. Mind & Language, 35(2), 209–223. https://doi.org/10.1111/mila.12281
Khalsa, S. S., Adolphs, R., Cameron, O. G., et al. (2018). Interoception and mental health: A roadmap. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging, 3(6), 501–513. https://doi.org/10.1016/j.bpsc.2017.12.004
Lane, R. D., Ryan, L., Nadel, L., & Greenberg, L. S. (2015). Memory reconsolidation, emotional arousal, and the process of change in psychotherapy: New insights from brain science. Behavioral and Brain Sciences, 38, e1. https://doi.org/10.1017/S0140525X14000041
LeDoux, J. E. (2015). Anxious: Using the brain to understand and treat fear and anxiety. Viking.
Marx, W., Moseley, G., Berk, M., & Jacka, F. (2017). Nutritional psychiatry: The present state of the evidence. Proceedings of the Nutrition Society, 76(4), 427–436. https://doi.org/10.1017/S0029665117002026
Mirea, D. (2018, October 19). The underlayers of NeuroAffective-CBT®. NeuroAffective-CBT®. https://neuroaffectivecbt.com/2018/10/19/the-underlayers-of-neuroaffective-cbt/
Mirea, D. (2023, July 18). Tired, Exercise and Diet your way out of trouble: TED’s your best friend. NeuroAffective-CBT®. https://neuroaffectivecbt.com/2023/07/18/teds-your-best-friend/
Mirea, D. (2025, December 10). TED in NeuroAffective-CBT®: An applied self-regulation framework for enhancing emotional well-being through sleep, movement, and nutrition. NeuroAffective-CBT®. https://neuroaffectivecbt.com/2025/12/10/ted-in-neuroaffective-cbt-an-applied-self-regulation-framework-for-enhancing-emotional-well-being-through-sleep-movement-and-nutrition/
Mirea, D. (2025, December 17). The use of lifestyle interventions in psychotherapy. NeuroAffective-CBT®. https://neuroaffectivecbt.com/2025/12/17/the-use-of-lifestyle-interventions-in-psychotherapy/
Niedenthal, P. M. (2007). Embodying emotion. Science, 316(5827), 1002–1005. https://doi.org/10.1126/science.1136930
Panksepp, J. (1998). Affective neuroscience: The foundations of human and animal emotions. Oxford University Press.
Pessoa, L. (2017). A network model of the emotional brain. Trends in Cognitive Sciences, 21(5), 357–371. https://doi.org/10.1016/j.tics.2017.03.002
Phillips, K. A. (2005). The broken mirror: Understanding and treating body dysmorphic disorder (Rev. ed.). Oxford University Press.
Phillips, K. A., Didie, E. R., Feusner, J., & Wilhelm, S. (2008). Body dysmorphic disorder: Treating an underrecognized disorder. American Journal of Psychiatry, 165(9), 1111–1118. https://doi.org/10.1176/appi.ajp.2008.08040500
Seth, A. K., & Friston, K. J. (2016). Active interoceptive inference and the emotional brain. Philosophical Transactions of the Royal Society B: Biological Sciences, 371(1708), 20160007. https://doi.org/10.1098/rstb.2016.0007
Siegel, D. J. (2012). The developing mind: How relationships and the brain interact to shape who we are (2nd ed.). Guilford Press.
Veale, D. (2004). Advances in a cognitive behavioural model of body dysmorphic disorder. Body Image, 1(1), 113–125. https://doi.org/10.1016/S1740-1445(03)00009-3
Veale, D., & Neziroglu, F. (2010). Body dysmorphic disorder: A treatment manual. Wiley-Blackwell.
Wilhelm, S., Phillips, K. A., & Steketee, G. (2013). Cognitive behavioral therapy for body dysmorphic disorder: A treatment manual. Guilford Press.