

Daniel Mirea (May, 2026)
|The NeuroAffective-CBT® Journal |
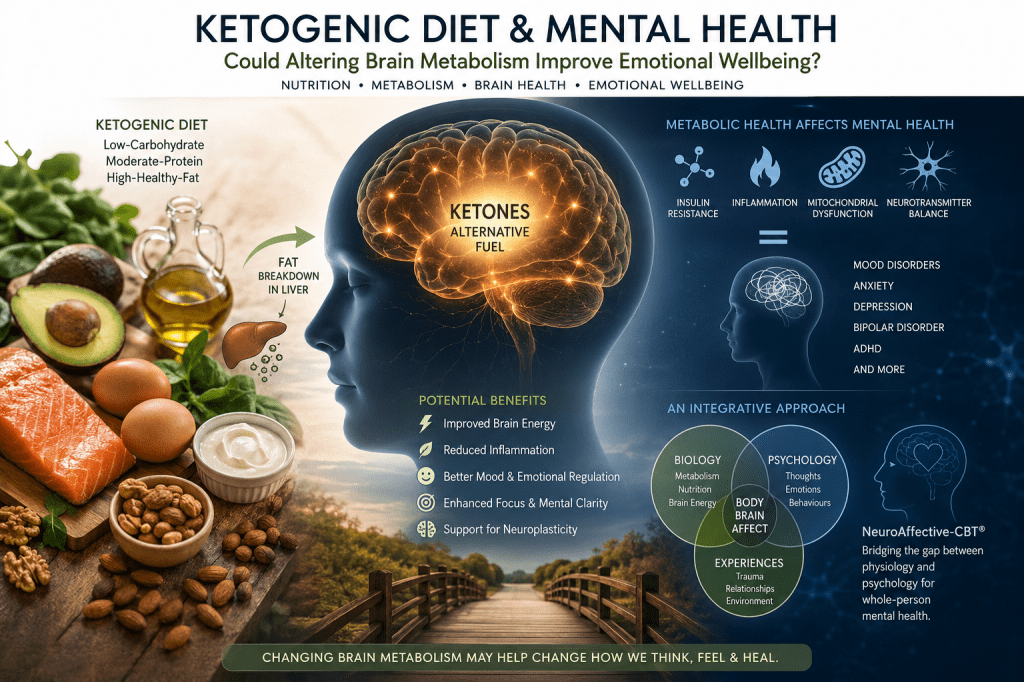
Could Altering Brain Metabolism Improve Emotional Wellbeing?
Abstract
This article explores the emerging fields of metabolic psychiatry and nutritional psychiatry, two rapidly developing areas of research investigating how metabolism, inflammation, insulin resistance, mitochondrial function, and nutrition may influence mental health and brain functioning. It examines the growing interest in ketogenic diets, originally developed in the 1920s as a treatment for epilepsy, as potential interventions capable of affecting mood, cognition, emotional regulation, and psychiatric symptoms through changes in brain energy metabolism.
The article also considers an important conceptual question: why are these developments increasingly discussed within psychiatry and medicine, yet far less frequently within mainstream psychology and psychotherapy? While nutritional psychiatry focuses upon the biological and medical relationship between diet and mental illness, psychological models have historically placed greater emphasis upon cognition, behaviour, trauma, attachment, and emotional learning. Emerging integrative approaches such as NeuroAffective-CBT® (NA-CBT®) attempt to bridge this divide by recognising that psychological functioning and physiological regulation continuously interact within the Body–Brain–Affect system.
Although research in this area remains in its early stages, increasing evidence suggests that mental health and metabolic health may be far more interconnected than previously understood.
The relationship between nutrition, metabolism, and mental health is increasingly recognised as one of the most important discussions within modern psychiatry and integrative psychotherapy.
Keywords:
Ketogenic diet; mental health; metabolic psychiatry; nutritional psychiatry; NeuroAffective-CBT; NA-CBT; brain metabolism; insulin resistance; mitochondrial dysfunction; emotional regulation; nutritional ketosis; psychotherapy; metabolism and mental health; inflammation; neuroplasticity; brain energy; metabolic health; depression; anxiety; bipolar disorder; ADHD; trauma; Body–Brain–Affect model.
Introduction: Exploring the Emerging Science of Metabolic Psychiatry
For decades, mental health treatment has focused primarily on psychotherapy and medication. These approaches remain incredibly important and, for many people, life-changing. However, a growing body of research is beginning to suggest that another major factor may have been underestimated for far too long:
Metabolic health.
Researchers working within the emerging field of metabolic psychiatry are increasingly exploring how brain energy, inflammation, insulin resistance, diet, and mitochondrial function may influence emotional wellbeing and psychiatric symptoms.
One of the most discussed interventions within this field is the ketogenic diet — not simply as a weight-loss strategy, but as a possible way of improving how the brain produces and uses energy.
At its core, the idea is surprisingly simple:
Mental health and physical metabolism may be far more interconnected than we once believed.
What Is the Ketogenic Diet?
The ketogenic diet was originally developed in the 1920s as a medical treatment for severe epilepsy in children. Physicians had noticed that periods of fasting sometimes dramatically reduced seizures, but prolonged fasting was obviously not sustainable. Researchers therefore attempted to create a diet that could reproduce the metabolic effects of fasting while still allowing people to eat normally.
The result became known as the ketogenic diet.
A ketogenic diet significantly reduces carbohydrates while increasing fat intake and maintaining moderate protein levels. This shifts the body away from relying primarily on glucose (sugar) for energy and toward burning fat and producing molecules called ketones.
This metabolic state is known as nutritional ketosis.
Ketones can act as an alternative fuel source for the brain, and many researchers now believe that this change in fuel supply may affect not only physical health, but also emotional and cognitive functioning.
In simple terms, a ketogenic diet is a low-carbohydrate, moderate-protein, high-fat nutritional approach designed to shift the body away from relying primarily on glucose (sugar) for energy and toward producing ketones as an alternative fuel source. Ketones are molecules produced by the liver through the breakdown of fat and can be used by the brain and body for energy.
In practical terms, ketogenic diets typically encourage foods such as oily fish, eggs, olive oil, avocado, nuts, seeds, natural full-fat dairy products, and unprocessed meats, while reducing foods high in sugar and refined carbohydrates such as sweets, sugary drinks, white bread, pastries, ultra-processed snacks, and heavily processed fast foods. Many clinicians and researchers also emphasise the importance of prioritising healthier fats and minimally processed foods rather than simply consuming large amounts of fat indiscriminately.
Therefore ketogenic diets are not about proteins over everything else. Protein intake on a ketogenic diet is generally calculated according to body weight rather than height. The formula is rather simple:
Protein (g/day) = Body Weight (Kg) × 1.2–1.75
Where:
➔ 1.2 g/kg = Sedentary individuals
➔ 1.4–1.6 g/kg = Most adults following a ketogenic diet
➔ 1.75 g/kg = Physically active individuals, older adults, or those seeking to preserve lean muscle mass
Example:
An individual weighing 80 kg would require:
80 kg × 1.2 = 96 g protein/day
to
80 kg × 1.75 = 140 g protein/day
Therefore, a daily protein intake of approximately 96–140 g of protein would be appropriate.
For individuals who are significantly overweight or obese, protein requirements may be calculated using ideal body weight or estimated lean body mass rather than total body weight.
Importantly, ketogenic diets are not high-protein diets. Therapeutic ketogenic approaches are typically characterised as high-fat, moderate-protein, and very-low-carbohydrate diets, with protein intake maintained at levels sufficient to preserve muscle mass while supporting nutritional ketosis.
The Forgotten Medical History of Keto
Although ketogenic diets have become fashionable in recent years, their origins are deeply medical rather than commercial.
The ketogenic diet was first formally introduced in 1921 at the Mayo Clinic by Dr. Russell Wilder. At the time, it was considered a serious neurological treatment rather than a lifestyle trend.
Throughout the 1920s and 1930s, ketogenic diets were widely used in hospitals to treat epilepsy, often with remarkable results. Interest later declined after anti-seizure medications became available in the 1940s and 1950s, largely because medication was easier to prescribe and commercially scalable.
For decades, ketogenic therapy remained mostly confined to treatment-resistant epilepsy.
Only in the past twenty years has scientific interest expanded again. Researchers are now exploring ketogenic and low-carbohydrate approaches in relation to obesity, insulin resistance, type 2 diabetes, Alzheimer’s disease, Parkinson’s disease, migraine disorders, inflammation, and increasingly, mental health conditions such as depression, bipolar disorder, schizophrenia, anxiety disorders, and ADHD.
This newer field, more established in the United States than in the United Kingdom, is often referred to as metabolic psychiatry, a field that has emerged more recently than nutritional psychiatry. Using modern neuroscience and advances in brain metabolism research, it is beginning to revisit an old question:
Could changing brain metabolism influence mental health outcomes?
The Brain Is an Energy-Hungry Organ
The human brain represents only around 2% of total body weight, yet it consumes roughly 20% of the body’s energy at rest.
In simple terms, the brain is extraordinarily energy-demanding.
Increasingly, researchers suspect that many psychiatric and neurological conditions may involve problems with how the brain produces, accesses, or regulates energy. Scientists are investigating links between mental illness and insulin resistance, inflammation, oxidative stress, mitochondrial dysfunction, and disrupted neurotransmitter regulation.
This has led to an important question:
What happens when the brain is not being fuelled efficiently?
Some researchers now believe that certain psychiatric symptoms may partly reflect a “brain energy crisis” occurring at the cellular level.
“Changing the Brain’s Operating System”
Harvard psychiatrist Chris Palmer has described the ketogenic diet as potentially changing the brain’s “operating system.”
When the body moves away from a high-carbohydrate, high-insulin state and begins using ketones for fuel, brain cells appear to function differently. Researchers believe this metabolic shift may influence inflammation, neurotransmitter balance, oxidative stress, hormone regulation, and mitochondrial function.
Some scientists hypothesise that ketones may provide a more stable and efficient fuel source for certain brain cells, potentially improving energy production while reducing inflammatory stress.
Although the science is still evolving, this may help explain why some individuals report improvements not only in weight or energy levels, but also in mood stability, concentration, emotional regulation, and mental clarity.
Mental Health and Metabolic Dysfunction
Modern psychiatry is increasingly recognising that mental health difficulties are not always “just psychological.”
Large studies have repeatedly found strong associations between psychiatric conditions and metabolic problems such as obesity, insulin resistance, metabolic syndrome, inflammation, and type 2 diabetes.
This does not mean that depression, anxiety, bipolar disorder, ADHD, PTSD, or schizophrenia are “caused by diet.” Mental health is always complex and multi-layered. Trauma, relationships, stress, genetics, attachment history, and social environment all matter enormously.
However, biology matters too.
In fact, poor metabolic health may sometimes worsen emotional regulation, cognitive function, fatigue, motivation, sleep quality, and stress resilience. To complicate matters further, many psychiatric medications themselves can contribute to weight gain, insulin resistance, and metabolic dysfunction.
Whilst much of the emerging ketogenic psychiatry literature has focused upon symptom reduction, an equally important question may be whether metabolic interventions influence a person’s ability to engage with psychotherapy itself. This issue is particularly relevant within NeuroAffective-CBT (NA-CBT), where emotional regulation, cognitive flexibility, behavioural activation, and trauma processing are understood as dependent upon the ongoing interaction between physiology, affect, and cognition within the Body–Brain–Affect system.
Ketogenic Diets and Psychotherapy Engagement: A NeuroAffective-CBT Perspective
Recent work by Laurent (2026) has proposed an important conceptual shift in how ketogenic metabolic therapy (KMT) may be understood within mental health services. Rather than focusing solely on whether ketogenic interventions directly reduce psychiatric symptoms, Laurent suggests that an equally important question is whether metabolic stabilisation may improve a person’s capacity to engage with psychotherapy itself.
Writing specifically about Cognitive Behavioural Therapy for Psychosis (CBTp), Laurent highlights that many individuals struggle to fully participate in treatment because of factors such as sleep disturbance, cognitive overload, emotional reactivity, poor concentration, low distress tolerance, fluctuating motivation, and difficulties completing between-session therapeutic tasks. These barriers often interfere with treatment initiation, retention, and successful completion.
As Laurent explains:
“The question of this paper is not whether ketogenic therapies are an effective treatment for schizophrenia spectrum disorders. The question is whether this can improve the ability for these patients to utilise CBTp.“
This distinction is clinically significant because it shifts attention from symptom reduction alone towards the broader issue of therapeutic readiness and engagement. Rather than asking whether ketogenic metabolic therapy directly treats psychosis, Laurent asks whether improvements in physiological functioning may help individuals engage more effectively in the psychological work required for meaningful change.
During discussion of the paper, Laurent further observed:
“Could some of the treatment benefits that people are reporting map onto what patients talk about when they discuss having difficulty using CBT?“
This question closely mirrors one of the central assumptions underpinning NeuroAffective-CBT: that psychological change is influenced not only by what individuals think, but also by the physiological state from which those thoughts emerge. Improvements in sleep quality, energy regulation, metabolic functioning, emotional stability, and cognitive clarity may influence therapeutic outcomes not merely through symptom reduction, but by enhancing a person’s capacity to engage in emotional learning, behavioural change, cognitive restructuring, trauma processing, and the development of an integrated sense of self.
Within NA-CBT, therapeutic progress is not viewed solely as a product of cognitive insight. Psychological functioning is understood as emerging from the continuous interaction between physiological regulation, emotional processing, and cognitive interpretation, as illustrated within the Body–Brain–Affect Triangle. From this perspective, interventions that improve physiological stability may indirectly strengthen psychotherapy by creating the conditions necessary for reflective thinking, emotional regulation, behavioural activation, and psychological resilience.
Laurent identifies several domains repeatedly reported within the ketogenic psychiatry literature that are also recognised barriers to successful psychotherapy engagement:
- Sleep disturbance
- Cognitive burden and “brain fog”
- Emotional distress reactivity
- Mood instability
- Reduced resilience
- Functional impairment in everyday life
These domains overlap considerably with those addressed within the original NeuroAffective-CBT® TED model (Tiredness–Exercise–Diet), where physiological regulation is viewed as a prerequisite for optimal emotional and cognitive functioning.
This observation is particularly noteworthy because the original TED model was developed long before the recent emergence of metabolic psychiatry. TED was originally conceived as a practical psychoeducational framework helping clients understand how tiredness, physical activity, nutrition, and lifestyle behaviours continuously influence emotional regulation, cognitive functioning, decision-making, and psychological resilience. From an NA-CBT® perspective, physiological dysregulation frequently manifests as emotional volatility, cognitive overload, reduced distress tolerance, motivational difficulties, and increased vulnerability to shame-based coping patterns. The emerging ketogenic psychiatry literature may therefore be viewed as supporting a broader principle already embedded within the TED framework: when physiology becomes more stable, emotional regulation improves, cognitive flexibility increases, and psychological change often becomes more accessible.
From an NA-CBT perspective, ketogenic interventions should not be viewed as replacements for psychotherapy. Rather, where clinically appropriate and medically supervised, they may function as adjunctive interventions that enhance readiness for psychological treatment. In other words, metabolic interventions may help prepare the psychological and physiological conditions in which psychotherapy can take root and flourish.
This perspective is consistent with a broader biopsychosocial understanding of mental health. When physiological dysregulation is reduced, individuals often experience improved concentration, greater emotional tolerance, increased motivation, enhanced self-reflective capacity, and greater resilience in the face of distress. These changes may allow them to engage more effectively with cognitive restructuring, behavioural experiments, trauma processing, emotional regulation work, and other psychotherapy interventions.
Future research will be needed to determine the extent to which ketogenic metabolic therapy improves psychotherapy engagement across a range of mental health conditions. Nevertheless, the emerging evidence reinforces an important principle already embedded within the NeuroAffective-CBT framework: sustainable psychological change is often easier to achieve when physiological regulation is addressed alongside emotional and cognitive processes. Put simply, when the body functions more effectively, the mind is often better positioned to learn, adapt, regulate, and heal.
Within the NeuroAffective-CBT Body–Brain–Affect Triangle, physiological regulation, emotional experience, and cognitive processing are viewed as continuously interacting components of a single integrated system. Changes in sleep quality, nutrition, inflammation, insulin sensitivity, hormonal balance, physical activity, and energy metabolism do not simply affect the body; they may also influence how emotions are experienced, how meaning is constructed, and how individuals respond to psychological challenges.
From this perspective, ketogenic metabolic therapy represents one example of a broader principle that has long been embedded within the NA-CBT framework: psychological functioning cannot be fully separated from physiological functioning. The way we think, feel, regulate emotions, tolerate distress, and engage in psychotherapy is influenced not only by our beliefs, learning history, and relationships, but also by the biological state of the nervous system from which those experiences emerge.
Consequently, interventions that improve physiological regulation may indirectly enhance emotional resilience, cognitive flexibility, distress tolerance, self-reflective capacity, and therapeutic engagement. From a NeuroAffective-CBT perspective, physiology and psychology are not separate domains competing for explanatory power; rather, they represent different levels of the same interconnected human system. The Body–Brain–Affect Triangle therefore provides a framework for understanding how changes in metabolism, sleep, nutrition, physical activity, emotional regulation, cognition, behaviour, and relationships continuously influence one another. In this context, ketogenic metabolic therapy may be viewed not simply as a dietary intervention, but as one potential pathway through which physiological stabilisation may facilitate emotional regulation, psychological growth, and meaningful therapeutic change.
Clinical Implications for NeuroAffective-CBT
As discussed previously in the article TED Series, Part II: Insulin Resistance and Mental Health, insulin resistance may influence far more than blood sugar alone. Emerging evidence suggests it may also contribute to fatigue, emotional instability, cognitive slowing, cravings, depressive symptoms, and motivational collapse.
Within the NeuroAffective-CBT framework, these physiological states are understood as directly influencing the Body–Brain–Affect system central to emotional functioning.
From this perspective, ketogenic diets may hold psychotherapeutic relevance because they target metabolic flexibility and glucose regulation. By reducing glucose volatility and lowering insulin demand, ketogenic interventions may help stabilise energy availability within the brain and nervous system.
In everyday clinical terms, this may mean that some individuals feel calmer, clearer, less reactive, more emotionally stable, and more capable of engaging in therapeutic work.
Within NA-CBT, TED interventions (Tired–Exercise–Diet) are not presented as rigid dietary rules or wellness ideology. Rather, they are viewed as biologically informed interventions that may improve emotional regulation capacity and psychotherapy responsiveness.
When individuals experience chronic fatigue, emotional dysregulation, shame-driven eating, unstable sleep, poor concentration, or constant cravings, psychotherapy itself may become significantly more difficult because the nervous system remains physiologically overwhelmed.
Chronic physiological dysregulation may also increase vulnerability to shame-based interpretations of failure, weakness, inadequacy, and self-criticism, further reinforcing the maladaptive cycles described within the Pendulum Effect model of NeuroAffective-CBT.
Improving metabolic stability may therefore increase a person’s ability to tolerate emotions, engage in trauma processing, participate in behavioural activation, and benefit from cognitive restructuring.
Importantly, NA-CBT does not present ketogenic diets as a miracle cure or replacement for psychotherapy, psychiatric care, or medication. Rather, the model proposes that psychological functioning and physiological functioning continuously interact.
The brain does not operate separately from the body.
Emotional suffering is often both psychological and physiological at the same time.
Final Thoughts
The ketogenic diet is not a universal solution, and the science surrounding metabolic psychiatry remains in its early stages. Much more high-quality research is still needed, particularly regarding long-term outcomes, individual differences, and the interaction between nutrition, metabolism, psychotherapy, and psychiatric care.
However, one of the most important developments emerging from both metabolic psychiatry and nutritional psychiatry may be the growing recognition that mental health cannot be fully separated from physical health.
What we eat influences how we think, feel, regulate emotion, tolerate stress, and engage with the world around us. Brain metabolism, inflammation, insulin resistance, sleep, trauma, lifestyle, and emotional learning may all interact far more dynamically than traditional models once assumed.
At the same time, these developments raise important questions for psychology and psychotherapy. If nutrition and metabolism can influence mood, cognition, motivation, emotional regulation, and neuroplasticity, then psychological therapies may also benefit from greater integration with physiology and lifestyle medicine.
Approaches such as NeuroAffective-CBT (NA-CBT) attempt to bridge this divide by recognising that the brain does not operate separately from the body, and emotional suffering is often simultaneously psychological, neurological, behavioural, and physiological.
Rather than viewing biology and psychology as competing explanations, emerging integrative models increasingly suggest they may represent different levels of the same human system.
The future of mental health treatment may therefore lie not in choosing between biology or psychology, but in understanding how physiology, emotion, cognition, behaviour, relationships, trauma, and meaning continuously interact within one integrated human system. From a NeuroAffective-CBT perspective, lasting psychological change becomes most achievable when the Body, Brain, and Affect are understood not as separate domains, but as interconnected components of the same human experience.
Disclaimer
This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Ketogenic diets and therapeutic nutritional ketosis may significantly affect metabolism, medications, blood sugar, blood pressure, and psychiatric symptoms. Individuals considering significant dietary changes, particularly those with mental health conditions, eating disorders, diabetes, or those taking medication, should consult appropriately qualified healthcare professionals before making changes to diet or treatment plans.
References
Chris Palmer (2022). Brain Energy: A Revolutionary Breakthrough in Understanding Mental Health — and Improving Treatment for Anxiety, Depression, OCD, PTSD, and More. BenBella Books.
Georgia Ede (2024). Change Your Diet, Change Your Mind. London: Hodder & Stoughton.
Laurent, N. (2026) ‘Ketogenic metabolic therapy as a candidate adjunct for CBTp delivery in schizophrenia spectrum disorders’, Frontiers in Psychology, 17, 1775511. doi:10.3389/fpsyg.2026.1775511.
Mirea, D. (2025) TED in NeuroAffective-CBT®: An applied self-regulation framework for enhancing emotional well-being through sleep, movement and nutrition. NeuroAffective-CBT®. Available at: https://neuroaffectivecbt.com/2025/12/10/ted-in-neuroaffective-cbt-an-applied-self-regulation-framework-for-enhancing-emotional-well-being-through-sleep-movement-and-nutrition/ (Accessed: 2026).
Russell Wilder (1921). Original work introducing the ketogenic diet as a treatment for epilepsy at the Mayo Clinic.
Further Reading
Articles exploring NeuroAffective-CBT®, emotional regulation, trauma, neuroplasticity, and the Body–Brain–Affect model. And additional perspectives integrating physiology and psychotherapy can be found at NeuroAffective-CBT® Articles including: TED Series, Part II: Insulin Resistance and Mental Health
Research literature within Metabolic Psychiatry exploring the relationship between brain energy metabolism, insulin resistance, inflammation, and psychiatric disorders.
Mitochondrial Psychiatry literature investigating the role of mitochondrial dysfunction in depression, bipolar disorder, schizophrenia, and neurodegenerative conditions.
Research into insulin resistance and mental health increasingly suggests associations between impaired glucose metabolism, inflammation, depression, cognitive dysfunction, and emotional dysregulation.
Studies investigating ketogenic therapy in epilepsy continue to demonstrate the long-established neurological effects of nutritional ketosis, particularly in treatment-resistant epilepsy.
Evidence supporting ketogenic diet as an adjunct therapy in the treatment for chronic mental illness:
