NeuroAffective-CBT® is a cutting-edge evolution in psychotherapy, integrating the structured methods of traditional behaviourism with a deeper understanding of human physiology and emotional processing. The brain, working with the mind, constantly predicts and strategises with one core purpose: keeping the body alive. By recognising the intricate interplay between thought, emotion and neurobiology, NA-CBT® offers a nuanced and effective framework for addressing deep-seated emotional difficulties.
Pain is not simply a signal travelling from the body to the brain. It is a neuroaffective experience emerging from the continuous interaction between physiology, emotion, cognition, and context.
Pain has traditionally been conceptualised as a direct consequence of tissue damage, whereby nociceptive signals travel from the body to the brain and are subsequently perceived as pain. However, contemporary neuroscience suggests that this explanation is incomplete. Modern pain science increasingly recognises pain as a multidimensional neurobiological and psychological experience that emerges from the continuous interaction between sensory information, emotional states, memory, learning, expectation, context, and prediction. This article explores the distinction between nociception and pain, reviews the role of spinal gating and descending modulation pathways, and examines how affective and cognitive processes contribute to the conscious experience of pain. Drawing upon developments in affective neuroscience, cognitive neuroscience, and contemporary pain research, the article proposes that pain is best understood as a neuroaffective phenomenon rather than a simple sensory event. A NeuroAffective-CBT® (NA-CBT®) perspective is presented, conceptualising pain as the product of an ongoing interaction between the body, brain, and affective systems. Understanding pain through this integrative framework may help clinicians and individuals alike appreciate why pain can persist in the absence of ongoing tissue damage and why effective treatment often requires a biopsychosocial and neuroaffective approach.
Although pain has been extensively studied within medicine, neuroscience, and rehabilitation disciplines, discussions within psychotherapy have often focused primarily on symptom management rather than on understanding pain as a complex neuroaffective experience. From a NeuroAffective-CBT perspective, this distinction is important because many of the emotional difficulties presented in therapy involve physiological distress that is experienced, interpreted, and responded to in ways that closely resemble the mechanisms observed in pain itself.
Therefore, pain is not simply something we detect. It is something we experience. And experiences emerge from the continuous conversation between the body, the brain, and affect.
Most of us have been taught a relatively simple explanation of pain. You step on a nail. The injured tissue sends a pain signal through the nerves. The signal travels up the spinal cord.
The brain receives the message. You feel pain.
Simple. Logical. Intuitive.
And yet, although this explanation contains some truth, it is only part of the story.
Over the last several decades, advances in neuroscience, psychology, pain medicine, and affective neuroscience have fundamentally changed our understanding of pain. What we once believed to be a straightforward sensory process is now understood to be a far more complex interaction between the body, brain, emotions, memories, beliefs, expectations, and context.
In many ways, pain provides one of the clearest examples of how the body, brain, and affective systems continuously interact to shape our lived experience.
Most educational diagrams describe pain as a four-step process:
1. Detection of Potential Harm
Specialised nerve endings known as nociceptors detect potentially harmful stimuli such as:
Extreme heat
Excessive pressure
Tissue injury
Chemical irritation
These receptors are often described as “pain receptors,” although this is not entirely accurate.
Their actual role is to detect potential danger.
When activated, they send electrical signals through peripheral nerves toward the spinal cord.
2. The Spinal Gate
The signal reaches the spinal cord, where information is filtered before continuing toward the brain.
This concept originates from the famous Gate Control Theory of Pain, proposed by Ronald Melzack and Patrick Wall in 1965.
According to this theory, the spinal cord functions somewhat like a gatekeeper.
Some signals are allowed through. Others are dampened. Others may be amplified.
This explains why rubbing an injured area often reduces discomfort. Touch signals can partially compete with and inhibit nociceptive input at spinal cord level.
3. Modulation
Signals reaching higher centres of the nervous system can be increased or decreased by descending pathways from the brainstem.
In some situations, pain can be dramatically suppressed.
Examples include:
Soldiers injured in battle
Athletes finishing a race despite serious injuries
Emergency situations where survival is prioritised
Conversely, pain can also be amplified by stress, anxiety, fear, sleep deprivation, inflammation, or sensitisation.
4. Conscious Perception
If sufficient information reaches the brain, pain becomes consciously experienced.
This is where most simplified diagrams end.
However, this is also where the most interesting part of the story begins.
The Biggest Misunderstanding About Pain
Perhaps the most important discovery in modern pain science is this:
Pain signals are not actually pain.
The nerves do not carry pain itself.
They carry information.
They carry evidence.
They carry warning signals.
What travels through the nervous system is better described as:
Nociception
Nociception refers to the detection and transmission of potentially harmful stimuli.
Pain, however, is something different.
Pain is an experience.
And experiences are generated by the brain.
This distinction may sound subtle, but it changes everything.
Nociception Without Pain
Consider the following examples.
A footballer breaks a bone during an important match and continues playing.
A soldier is shot in combat and reports little or no pain until reaching safety.
An individual involved in a car accident walks around helping others before realising they are injured.
In all these situations:
The injury exists.
The nociceptive signals exist.
Yet the pain experience is significantly reduced or absent. The nervous system has decided that survival is currently more important than suffering.
Pain Without Injury
Now consider the opposite situation.
An individual experiences severe chronic pain despite normal scans and medical investigations.
Someone develops phantom limb pain after amputation.
A person with fibromyalgia experiences widespread pain despite no obvious tissue damage.
An individual suffers debilitating migraines despite no visible injury.
In these situations, pain exists. Yet tissue damage may be minimal or absent. Again, pain cannot simply be explained as a direct readout of injury.
Something else is happening.
The Brain Is Not Reading Pain
A common misconception is that the brain acts like a computer reading incoming messages. The reality is far more sophisticated.
Modern neuroscience increasingly supports the idea that the brain functions as a prediction machine. Rather than passively waiting for information, the brain continuously asks:
“What is happening?”
“How dangerous is it?”
“What should I do about it?”
Pain appears to emerge from the brain’s attempt to answer these questions.
The human brain rapidly combines incoming sensory information with previous experiences, memory, learning, expectations, emotional state, beliefs, current stress levels, and environmental context before constructing the experience we call pain.
Pain is therefore not merely detected. Pain is actively constructed by the brain based upon incoming information, prior learning, emotional state, and context.
Why Context Matters
Imagine stepping on the same object under different circumstances.
Scenario One:
You are walking barefoot through your garden.
You step on a sharp object unexpectedly.
Pain is immediate.
Scenario Two:
You are undergoing a medical procedure.
You know discomfort is expected.
You trust the clinician.
The same level of stimulation may feel significantly less painful.
Scenario Three:
You are highly anxious, exhausted, sleep deprived, and worried about your health.
The exact same physical stimulus may feel dramatically worse.
The tissue has not changed.
The brain’s interpretation has changed.
The Emotional Brain and Pain
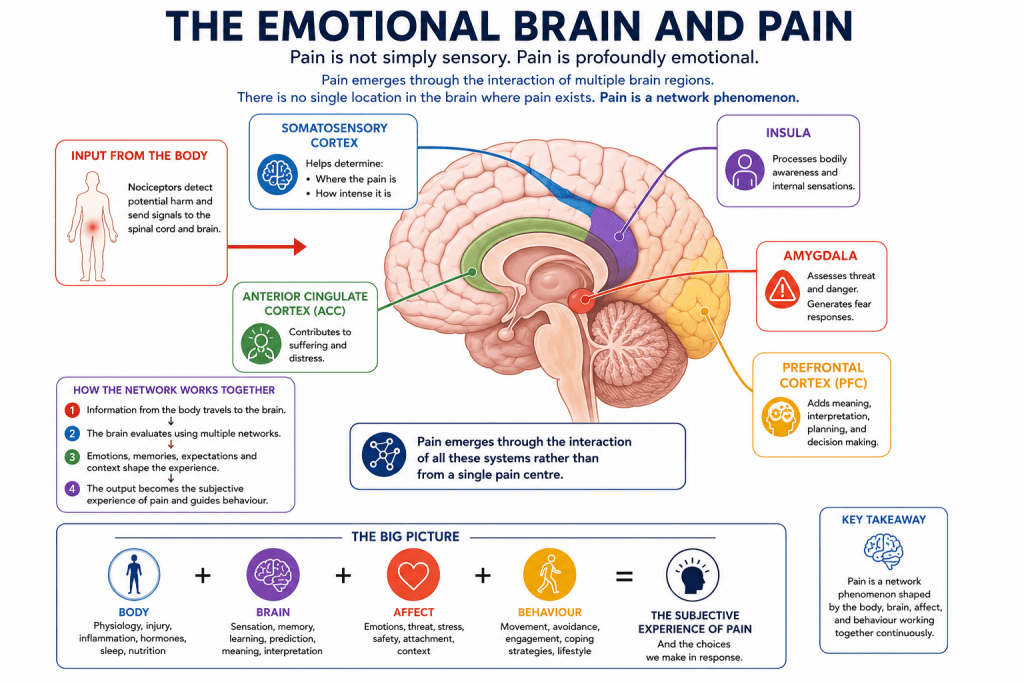
One of the greatest limitations of many pain models is that they largely ignore emotion. Pain is not simply sensory. Pain is profoundly emotional. Several brain regions contribute to the experience.
Somatosensory Cortex
Helps determine (1) Where the pain is (2) How intense it is
Insula
Processes bodily awareness and internal sensations.
Anterior Cingulate Cortex
Contributes to suffering and distress.
Amygdala
Assesses threat and danger.
Generates fear responses.
Prefrontal Cortex
Adds meaning, interpretation, planning, and decision making.
Pain emerges through the interaction of all these systems rather than from a single pain centre.
There is no single location in the brain where pain exists.
Pain is a network phenomenon.
Fear Can Increase Pain
Imagine touching a hot stove.
The immediate pain serves an adaptive purpose.
You withdraw your hand.
Problem solved.
However, if the nervous system begins associating many harmless experiences with danger, pain can become amplified.
The more fearful we become of pain:
The more we monitor it
The more we anticipate it
The more attention we give it
The more significant it can become.
This does not mean the pain is imaginary.
It means the nervous system is becoming increasingly protective.
In many chronic pain conditions, the alarm system becomes overly sensitive.
The danger detector becomes too good at its job.
What Chronic Pain Teaches Us
Acute pain protects us.
Chronic pain often reflects protection that has become excessive.
The nervous system learns.
The brain learns.
The body learns.
Neural pathways become strengthened through repetition.
Eventually the system may begin generating pain responses disproportionate to actual tissue damage.
This process is often referred to as:
Central sensitisation
Neural amplification
Pain sensitisation
The pain remains real.
The suffering remains real.
The underlying mechanisms, however, are different from those involved in acute injury.
A NeuroAffective-CBT Perspective
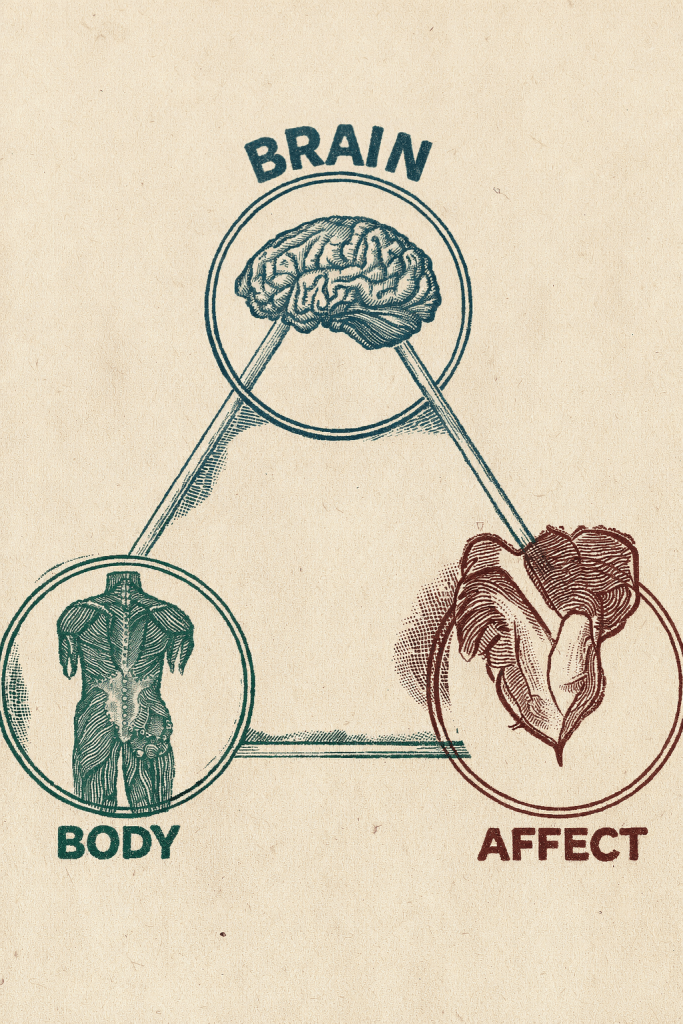
Within NeuroAffective-CBT, pain can be understood through the interaction between three continuously communicating systems:
Body
The body provides physiological information.
This includes:
Injury
Inflammation
Hormonal changes
Sleep quality
Nutrition
Energy availability
Physical conditioning
Brain
The brain interprets incoming information.
It generates predictions based upon:
Previous experiences
Memory
Learning
Core beliefs
Expectations
Affect
Affective systems shape emotional meaning.
These include:
Fear
Shame
Anxiety
Helplessness
Anger
Grief
Together these systems create the subjective experience we call pain.
Within NeuroAffective-CBT, emotional pain and physical pain are not viewed as entirely separate phenomena. Both involve physiological activation, affective meaning-making, cognitive interpretation, and behavioural responses. Clients frequently describe emotional suffering using physical language: a heavy chest, a knot in the stomach, emotional exhaustion, pressure, tension, emptiness, or feeling broken. Understanding pain therefore provides an important framework for understanding emotional suffering itself.
The Core Principle of NeuroAffective-CBT
The Body influences the Brain.
The Brain influences Affect.
Affect influences Behaviour.
Behaviour influences Physiology.
When any part of this system becomes dysregulated, suffering may emerge.
When all parts of the system are addressed together, healing becomes possible.
Why This Matters Clinically
Understanding pain differently changes how we approach treatment.
Rather than asking only:
“Where is the damage?”
We might also ask:
What is the nervous system trying to protect?
What role is stress playing?
What role is sleep playing?
What role is fear playing?
What role is emotional suppression playing?
What role is avoidance playing?
What role is physical deconditioning playing?
What role is chronic activation of threat systems playing?
These questions do not invalidate physical explanations.
They expand them.
Pain Is Real, Even When Scans Are Normal
One of the most harmful misconceptions encountered in clinical practice is the belief that normal scans mean symptoms are “all in the mind.”
Nothing could be further from the truth.
Modern neuroscience demonstrates that:
Pain is real.
The nervous system is real.
Brain-based processing is real.
Emotional amplification is real.
Sensitisation is real.
The absence of visible tissue damage does not invalidate suffering.
It simply means the explanation may be more complex than originally assumed.
The Future of Pain Science
Pain science continues to evolve.
Increasingly, researchers are recognising the importance of integrating:
Neuroscience
Psychology
Physiology
Immunology
Lifestyle medicine
Sleep science
Exercise science
Nutritional psychiatry
Metabolic psychiatry
into a more comprehensive understanding of human suffering.
Pain cannot be fully understood through tissue damage alone.
Nor can it be fully understood through psychology alone.
The future almost certainly lies in integration.
A NeuroAffective-CBT Formulation of Pain
From a NeuroAffective-CBT perspective, pain cannot be fully understood through a purely biomedical model, nor can it be adequately explained through a purely psychological framework. Rather, pain emerges from the dynamic interaction between physiological processes, affective systems, and cognitive interpretation. This perspective is consistent with the NA-CBT Body–Brain–Affect Triangle, which proposes that emotional and behavioural experiences arise from the continuous bidirectional communication between bodily states, brain-based processing, and affective meaning-making systems.
Within this framework, the body provides ongoing physiological information regarding injury, inflammation, fatigue, energy availability, sleep quality, nutrition, hormonal changes, and physical conditioning. The brain continuously interprets this information through the lens of prior learning, autobiographical memory, expectations, beliefs, and threat predictions. Simultaneously, affective systems assign emotional meaning to incoming experiences, influencing whether bodily sensations are perceived as manageable, threatening, overwhelming, or catastrophic.
Consequently, pain is not viewed as a simple readout of tissue damage but rather as a neuroaffective experience generated by the interaction of these multiple systems.
The Role of Threat Perception
One of the central assumptions within NA-CBT is that the nervous system is fundamentally organised around safety and survival. The brain continuously evaluates internal and external information to determine the level of threat present in any given situation.
When a stimulus is interpreted as dangerous, the nervous system may increase vigilance, muscular tension, autonomic arousal, and pain sensitivity. Conversely, when safety cues are present, physiological regulation improves, threat responses diminish, and pain intensity may decrease.
Importantly, threat perception is not determined solely by objective reality. It is influenced by previous experiences, trauma histories, attachment experiences, health beliefs, social context, and emotional states.
Two individuals may therefore experience the same physical injury in dramatically different ways depending upon how their nervous systems interpret and respond to the event.
Trauma, Emotional Learning, and Pain Amplification
Traumatic experiences can significantly alter the way the nervous system responds to future threats. Individuals who have experienced chronic adversity, abuse, neglect, medical trauma, bullying, or emotionally invalidating environments may develop heightened sensitivity within threat-detection systems.
Over time, the nervous system may become increasingly efficient at detecting danger, sometimes responding to relatively minor stimuli as though they represent significant threats.
Within the NA-CBT model, unresolved trauma memories may continue to influence present-day physiological and emotional reactions long after the original event has passed. Pain can therefore become linked not only to tissue-based signals but also to fear networks, emotional memories, learned associations, and protective behavioural patterns.
This perspective aligns with contemporary research demonstrating the involvement of the amygdala, anterior cingulate cortex, insula, hippocampus, and prefrontal regions in both pain processing and emotional regulation.
The Influence of Shame and Anxiety
NA-CBT places particular emphasis on the role of shame-based emotional schemas and chronic anxiety in maintaining emotional distress and self-sabotaging patterns.
Shame frequently operates as a hidden amplifier of suffering.
Individuals who carry longstanding beliefs such as:
“I am weak.”
“I should be coping better.”
“There must be something seriously wrong with me.”
“Nobody understands what I am going through.”
may experience increased emotional distress alongside physical symptoms.
Similarly, chronic anxiety can maintain heightened physiological arousal, increased muscle tension, sleep disruption, hypervigilance, and persistent monitoring of bodily sensations. These processes may inadvertently reinforce pain pathways and increase the perceived intensity of symptoms.
From a neuroaffective perspective, emotional suffering and physical suffering often become intertwined, creating self-reinforcing cycles that can be difficult to break without targeted intervention.
The Original TED Model: Tired, Exercise, and Diet
A central component of the NeuroAffective-CBT framework is the original TED model, which focuses on three fundamental physiological domains that frequently influence emotional wellbeing, stress tolerance, cognitive functioning, and pain perception:
Tiredness, Exercise, and Diet.
Within NA-CBT, TED is often conceptualised as an individual’s internal physiological coach. Before attempting to understand complex emotional reactions, trauma responses, self-sabotaging behaviours, or chronic distress, clinicians are encouraged to assess the extent to which these three biological domains may be influencing the individual’s current functioning.
Tiredness
Sleep deprivation and chronic fatigue can significantly alter the way the nervous system processes both emotional and physical experiences.
Research consistently demonstrates that insufficient sleep is associated with:
Increased pain sensitivity
Reduced emotional regulation
Heightened threat perception
Increased anxiety and irritability
Poorer stress tolerance
Reduced cognitive flexibility
Greater physiological arousal
From a neuroaffective perspective, an exhausted nervous system is often a more reactive nervous system.
Individuals experiencing chronic pain frequently report poor sleep quality, whilst poor sleep itself can increase pain intensity, creating a self-perpetuating cycle of distress and physiological dysregulation.
For this reason, improving sleep and recovery is often considered a foundational intervention within the NA-CBT model before attempting more intensive emotional processing work.
Exercise
Physical activity plays a critical role in both emotional and physiological regulation.
Regular movement influences multiple systems associated with pain modulation, including:
Endorphin release
Stress regulation
Neuroplasticity
Cardiovascular health
Inflammatory processes
Mood regulation
Self-efficacy and resilience
Importantly, exercise may also help challenge fear-avoidance patterns commonly observed in chronic pain conditions.
Many individuals gradually reduce activity levels because movement becomes associated with discomfort or fear of injury. Whilst avoidance may provide short-term relief, prolonged inactivity can contribute to deconditioning, increased vulnerability, reduced confidence, and further sensitisation of the nervous system.
Within NA-CBT, exercise is therefore viewed not simply as a physical intervention but also as a psychological and neurobiological regulator capable of influencing both mood and pain perception.
Diet
Nutrition provides the biological foundation upon which the brain and body operate.
Emerging evidence from nutritional psychiatry, metabolic psychiatry, and neuroscience increasingly suggests that dietary factors may influence emotional wellbeing, inflammation, energy production, cognitive functioning, and stress resilience.
Poor nutritional habits may contribute to:
Fatigue
Metabolic dysfunction
Increased inflammation
Blood sugar instability
Reduced concentration
Mood fluctuations
Poor recovery capacity
From an NA-CBT perspective, diet is not viewed through a restrictive or purely weight-focused lens. Rather, it is considered a crucial component of physiological regulation that may influence how effectively the nervous system responds to both emotional and physical stressors.
TED and Pain Perception
The relevance of the TED model to pain becomes increasingly apparent when viewed through a neuroaffective lens.
An individual who is:
Chronically sleep deprived,
Physically deconditioned,
Nutritionally dysregulated,
may experience a nervous system that is more reactive, more vigilant, and more sensitive to both internal and external stressors.
Consequently, pain intensity may increase even when tissue damage remains unchanged.
Conversely, improvements in sleep, physical conditioning, and nutritional stability may help reduce physiological stress, improve emotional regulation, increase resilience, and support healthier pain modulation pathways.
Within the NeuroAffective-CBT framework, TED therefore represents far more than a lifestyle intervention.
It represents a foundational physiological platform upon which emotional regulation, cognitive flexibility, behavioural change, trauma processing, and recovery can occur.
When individuals begin addressing tiredness, exercise, and diet simultaneously, they are often not simply improving their physical health. They are creating the biological conditions necessary for the nervous system to feel safer, more regulated, and less protective.
From this perspective, the TED model becomes directly relevant to understanding why some individuals remain trapped within cycles of chronic pain, emotional distress, and physiological dysregulation, whilst others gradually move towards recovery and resilience.
Metabolic Health, Ketogenic Therapies and Pain
Over recent years, growing attention has been directed towards the relationship between metabolic health, inflammation, brain function, emotional wellbeing, and chronic illness. Whilst traditionally associated with weight management or epilepsy treatment, ketogenic therapies are increasingly being investigated for their potential effects on neurological, psychiatric, and inflammatory conditions.
As discussed in a recent NeuroAffective-CBT article exploring ketogenic therapies and mental health, emerging research suggests that metabolic dysfunction may influence psychological wellbeing through mechanisms involving inflammation, mitochondrial function, oxidative stress, insulin resistance, and energy metabolism within the brain.
This perspective aligns closely with one of the central assumptions of the NA-CBT model: the brain does not function independently from the body. Physiological dysregulation may influence emotional wellbeing, whilst emotional distress may simultaneously influence physiological functioning.
The relevance of this emerging field to pain should not be underestimated.
Many chronic pain conditions are now recognised to involve not only structural or tissue-based factors but also inflammatory processes, autonomic dysregulation, altered stress responses, sleep disturbance, and changes in central nervous system functioning. Increasingly, researchers are exploring whether metabolic interventions may influence some of these mechanisms.
As stated in the recent NeuroAffective-CBT review of ketogenic therapies:
“The question is not whether ketogenic therapies represent a miracle cure. The question is whether some of the benefits reported by patients may be explained by improvements in physiological regulation, inflammation, energy metabolism, sleep, cognition, and emotional stability.”
This is an important distinction.
Within NA-CBT, ketogenic diets are not conceptualised as psychological treatments. Rather, they may represent one example of how physiological interventions can potentially influence the Body–Brain–Affect system.
For some individuals, improvements in metabolic health may be associated with:
Reduced systemic inflammation
Improved energy regulation
Enhanced cognitive clarity
Better sleep quality
Reduced emotional volatility
Improved stress tolerance
All of which may indirectly influence the experience of pain.
Further research is required before definitive conclusions can be reached. However, the growing field of metabolic psychiatry reinforces a principle that sits at the heart of NeuroAffective-CBT®:
The body influences the brain. The brain influences affect. Affect influences behaviour. Behaviour influences physiology.
Understanding pain therefore requires us to look beyond symptoms alone and consider the broader physiological and emotional ecosystem within which those symptoms occur.
Towards an Integrated Understanding of Pain
The clinical implications of this model are significant.
Rather than asking solely:
“Where is the injury?“
NA-CBT® encourages clinicians and individuals to also ask:
What is the nervous system trying to protect?
What emotional meanings have become attached to the symptoms?
What role is fear playing?
What role is shame playing?
What role is avoidance playing?
What role is trauma playing?
What role are sleep, nutrition, and physical conditioning playing?
What factors are maintaining the brain’s prediction that danger remains present?
These questions do not deny the reality of pain.
Instead, they acknowledge the complexity of human suffering and provide a broader framework for understanding why pain may persist long after tissue healing has occurred.
Ultimately, the NeuroAffective-CBT® model views pain as a whole-person experience emerging from the continuous interaction between the body, brain, and affective systems. By addressing all three domains simultaneously, clinicians may be better positioned to help individuals reduce suffering, improve functioning, and develop a more integrated relationship with their physical and emotional experiences.
Final Thoughts
Perhaps the most important lesson from modern pain science is this:
Pain is not simply a signal travelling from the body to the brain.
Pain is a dynamic neurobiological experience emerging from the continuous interaction between bodily information, emotional states, prior learning, memory, beliefs, context, and prediction.
The body provides information.
The brain evaluates that information.
The affective system gives it meaning.
Together they create the conscious experience we call pain.
Understanding this complexity does not make pain less real.
If anything, it helps explain why pain can sometimes persist long after tissue healing has occurred, why emotions can influence symptoms, why stress can worsen discomfort, and why genuinely effective treatment often requires us to address the whole person rather than a single body part.
In many respects, pain may be one of the clearest demonstrations that human beings cannot be reduced to either mind or body alone.
We are, and always have been, an integrated neuroaffective system.
References
Apkarian, A.V., Baliki, M.N. and Geha, P.Y. (2009) ‘Towards a theory of chronic pain’, Progress in Neurobiology, 87(2), pp. 81–97.
Atlas, L.Y. and Wager, T.D. (2012) ‘How expectations shape pain’, Neuroscience Letters, 520(2), pp. 140–148.
Craig, A.D. (2003) ‘A new view of pain as a homeostatic emotion’, Trends in Neurosciences, 26(6), pp. 303–307.
Eccleston, C. and Crombez, G. (1999) ‘Pain demands attention: A cognitive-affective model of the interruptive function of pain’, Psychological Bulletin, 125(3), pp. 356–366.
Fields, H.L. (2004) ‘State-dependent opioid control of pain’, Nature Reviews Neuroscience, 5(7), pp. 565–575.
Flor, H. (2003) ‘Cortical reorganisation and chronic pain: Implications for rehabilitation’, Journal of Rehabilitation Medicine, 35(S41), pp. 66–72.
Gatchel, R.J., Peng, Y.B., Peters, M.L., Fuchs, P.N. and Turk, D.C. (2007) ‘The biopsychosocial approach to chronic pain: Scientific advances and future directions’, Psychological Bulletin, 133(4), pp. 581–624.
LeDoux, J.E. (2015) Anxious: Using the Brain to Understand and Treat Fear and Anxiety. New York: Viking.
Melzack, R. (1999) ‘From the gate to the neuromatrix’, European Journal of Pain, 3(Suppl A), pp. 121–126.
Melzack, R. and Wall, P.D. (1965) ‘Pain mechanisms: A new theory’, Science, 150(3699), pp. 971–979.
Mirea, D. (2018) Describing NeuroAffective-CBT®: An integrative model of psychological distress and emotional regulation. NeuroAffective-CBT®. Available at: https://neuroaffectivecbt.com (Accessed: 1 June 2026).
Mirea, D. (2026) Could altering brain metabolism improve emotional wellbeing? Exploring ketogenic therapies through a NeuroAffective-CBT® lens. NeuroAffective-CBT®. Available at: https://neuroaffectivecbt.com (Accessed: 1 June 2026).
A clinical story about how panic, shame, and physiological dysregulation interact and why stabilising physiological regulation can be the first step toward recovery.
When Jenna, a 26-year-old married woman, first arrived for therapy after the sudden onset of panic attacks, she dreaded that the conversation would revolve around her anxiety symptoms.
Naturally, she thought there would be questions about panic, about the frightening episode that had sent her to the emergency department, about what she had been thinking and feeling when the dizziness first appeared. In fact, she later admitted that she even anticipated she might throw up again.
What Jenna did not anticipate was that the assessment would begin somewhere more fundamental: examining the biological foundations that shape how the body responds to stress.
Sleep. Daily routines. Caffeine intake. Hydration. Movement. Even blood tests.
Like many people seeking help for panic attacks, Jenna assumed therapy would focus mainly on her thoughts, behaviours, and fears. Many people now research treatment options online before beginning therapy, and when they do, cognitive-behavioural methods such as interoceptive exposure are often presented as key evidence-based interventions, though they can also appear challenging at first.
What Jenna did not expect was that we would begin somewhere safer and more stabilising.
In the early sessions, rather than immediately exploring painful memories or emotional narratives, the work focused on regulation, restoring physiological balance through better sleep, movement, and nutritional habits.
The deeper personal stories would come later. Timing in NA-CBT is everything.
This approach reflects a core principle of NeuroAffective-CBT: when physiological arousal remains chronically elevated, emotional processing becomes far more difficult. Stabilising the body first often creates the conditions necessary for deeper psychological work to emerge safely.
Jenna had self-referred for therapy after a sudden episode of dizziness that appeared without warning two months earlier. The sensation was intense and frightening, accompanied by nausea, weakness in her knees, and a powerful fear that she might collapse or lose control. She went to the emergency department, where a full medical assessment was carried out. Neurological and vestibular causes were investigated, but no medical explanation was found.
Although the doctors reassured her that nothing serious had been detected, Jenna did not feel reassured. If anything, the uncertainty intensified her distress.
In the weeks that followed, panic attacks began to occur repeatedly. She developed a growing mistrust of her own body. Ordinary sensations—dizziness, nausea, shifts in breathing—began to feel unpredictable and dangerous. Her attention became increasingly focused inward, scanning constantly for signs that another episode might occur.
Soon the panic spread into daily life. Jenna began avoiding leaving the house alone. Shopping trips felt unsafe unless her husband accompanied her. Her world gradually narrowed as the fear of bodily sensations expanded.
Vomiting episodes also began to appear, usually during periods of intense anticipatory anxiety. These episodes seemed to provide temporary relief from the overwhelming sensations in her body, but they reinforced her belief that something was fundamentally wrong internally.
At the same time, sleep became disrupted. Fatigue increased. The body’s resilience decreased. The more exhausted she became, the more reactive her internal regulation felt.
During one of the early sessions, Jenna used a phrase that captured the essence of her distress:
“My body doesn’t feel safe anymore”.
At first glance, this presentation might seem like a relatively typical panic disorder with agoraphobic avoidance. But as the assessment unfolded, a deeper pattern began to emerge.
Jenna had been raised by a single mother together with three siblings. One memory stood out vividly. She was eight years old when her father left to work abroad and never returned. From that point forward, the emotional and practical responsibilities within the family shifted dramatically. Her mother, struggling with depression, found it difficult to maintain stability at home.
Jenna stepped in.
Even as a child, she assumed responsibilities that extended far beyond ordinary expectations. Helping her siblings became part of daily life, preparing lunches, supporting routines like cleaning and cooking and managing various responsibilities within the household.
Failure was not an option.
Getting things wrong felt dangerous. Someone might suffer if she did.
Looking back, Jenna described that period not as a conscious decision but as something she simply had to do. Over time, a quiet internal rule formed: if she remained alert enough, responsible enough, and careful enough, she could prevent things from going wrong.
The NeuroAffective-CBT formulation known as the Pendulum-Effect helps explain how such internal rules can shape coping patterns across many years.
At the centre of this pendulum system typically lies a powerful core affect—often shame, guilt, or the fear of failing others. Around this core experience, a set of self-protective strategies gradually develops in an attempt to manage the internal threat it creates.
In Jenna’s case, these strategies took three familiar forms. What once began as adaptive coping gradually evolved into self-sabotaging patterns that maintained the very distress they were originally designed to regulate.
One was overcompensation. She became highly vigilant, attentive to details, and constantly alert to potential problems. Missing something important felt unacceptable. Remaining on guard all the time seemed like the safest option.
Another strategy was avoidance. Situations that might create additional stress or draw attention toward her own needs were often postponed or abandoned. Investing time in herself, hobbies, rest, or personal interests, rarely felt justified.
Eventually, these cycles led to capitulation, moments when exhaustion and self-criticism took over. When she could not meet the impossible standards she had set for herself, the internal response was harsh: self-blame, guilt, and a sense that she was failing.
These strategies oscillated continuously—overcompensation, avoidance, and capitulation—like the movement of a pendulum. Each provided temporary relief from the underlying fear of getting things wrong, yet each also reinforced the deeper shame driving the system.
For many years, this pattern functioned quietly in the background of Jenna’s life.
Until her body interrupted it.
When panic attacks appeared, the same pendulum dynamics intensified. Hypervigilance shifted toward internal sensations. Avoidance expanded into everyday life. Exhaustion and self-criticism deepened when symptoms seemed uncontrollable.
This was one of the reasons the therapist introduced the TED framework (Tired–Exercise–Diet) early in the treatment process. Lifestyle interventions in NeuroAffective-CBT are not simply recommendations for general wellbeing. They function as direct interventions within the pendulum system itself.
For someone whose life has been dominated by overcompensation and self-neglect, improving sleep, eating regularly, or creating space for physical movement becomes more than self-care. It becomes a challenge to the internal rule that personal needs must always come last.
In Jenna’s case, stabilising her daily rhythms began to soften the relentless cycle of hypervigilance and exhaustion. Less fatigue meant less physiological reactivity. More predictable routines meant her internal regulation no longer had to remain constantly on guard.
Only once this stabilisation began did the deeper emotional narratives gradually come into view.
And only then did it become clear that Jenna’s panic attacks were not simply about panic.
They were about a system that had spent many years trying not to fail anyone, until eventually the pendulum could no longer keep swinging.
To understand why this happens, we need to look more closely at how panic attacks actually develop inside the body.
Why Panic Attacks Are Sometimes Not Just About Panic
When people experience their first panic attack, it often feels as though something in the body has suddenly gone wrong.
The heart races. Breathing changes. The body may tremble or feel weak. Dizziness appears without warning. Nausea, heat, or a sense of losing control can follow within seconds. Because these sensations are so intense and unfamiliar, many people understandably assume they are experiencing a serious medical emergency.
Jenna’s experience began in exactly this way.
The sudden dizziness that sent her to the emergency department felt like something catastrophic was happening inside her body. Even after medical tests ruled out neurological or vestibular causes, the feeling of danger did not disappear. The absence of a medical explanation did not bring relief, it created uncertainty.
And uncertainty is something the body’s regulatory system does not tolerate well.
From the outside, panic attacks can appear sudden and unpredictable. Yet when we look more closely, they often emerge from an internal system that has been under pressure for a long time.
NeuroAffective-CBT approaches panic from the understanding that emotional distress rarely originates in thoughts alone. Instead, it arises from the interaction between three continuously communicating systems: the body, the brain, and affect, our emotional signalling system.
The body constantly sends signals about internal states, fatigue, hunger, hormonal shifts, blood sugar levels, sleep deprivation, muscle tension, and breathing patterns. The brain interprets these signals and attempts to predict whether the environment is safe or threatening. Affect provides the emotional tone that guides behaviour: fear, shame, anger, safety, and relief.
When these systems are balanced, signals move smoothly between them. The body senses changes, the brain interprets them accurately, and emotions guide appropriate responses.
But when the system becomes dysregulated, those signals can begin to amplify one another.
Fatigue may increase physiological sensitivity. Increased sensitivity can heighten attention toward bodily sensations. Heightened attention can make normal sensations feel unusual or threatening. Once the brain interprets those sensations as danger, the body responds with a rapid stress reaction.
At that point, the panic attack is already underway.
In Jenna’s case, the first episode of dizziness acted like a spark in a system that was already vulnerable. Her autonomic state had spent many years in heightened vigilance, trying to anticipate problems, trying not to miss anything important, trying not to fail the responsibilities she had carried since childhood.
Hypervigilance can be a powerful survival strategy. It helps people remain alert, organised, and prepared. But when the body remains in this state for too long, it becomes increasingly sensitive to internal signals.
Even small fluctuations in breathing, blood pressure, or balance can suddenly feel alarming.
The body begins sending signals of danger not because there is a real external threat, but because the regulatory system has become overly reactive.
Once that cycle begins, panic attacks can develop quickly. The body senses something unusual, the brain interprets it as threat, and the emotional system amplifies the response.
This is why panic attacks often persist even when people know intellectually that nothing medically dangerous is happening.
The mind may understand that the body is safe, but the body’s internal regulation has not yet learned that lesson.
And this is also why treatment that focuses only on thoughts may not always be sufficient.
If the body remains exhausted, overstimulated, sleep deprived, or metabolically unstable, it will continue sending signals that the brain interprets as danger. The emotional system then reacts accordingly.
In other words, the panic attack may be the final expression of a much larger regulatory imbalance.
This was the case for Jenna.
Her panic attacks were not simply the result of catastrophic thinking about bodily sensations. They were emerging from a system that had been operating under prolonged pressure, physiologically, emotionally, and psychologically.
Before the deeper emotional narratives could be explored, her body first needed something much more basic. It needed stabilisation.
And that is why, in the early sessions of therapy, the focus turned toward something Jenna had not expected to discuss at all, how she slept, how she ate, how she moved, and how her body had been carrying the weight of many years of responsibility.
The next step was learning something much harder: how to experience safety again inside her own body.
Learning to Trust the Body Again
Understanding the pendulum was an important step for Jenna.
But understanding alone was not enough.
Her mind could now see the pattern, how vigilance, avoidance, and self-criticism had reinforced one another for years, but her body was still reacting as if danger could appear at any moment. The dizziness, the nausea, the waves of anxiety still felt unpredictable.
And unpredictability is exactly what keeps the nervous system on guard. So the next phase of therapy focused on something very practical: helping Jenna experience safety again inside her own body. This required gently reversing several habits that had developed since the panic attacks began.
One of the most powerful of those habits was constant monitoring of internal sensations. Jenna had become extremely attentive to what was happening inside her body. Small changes in balance, breathing, or stomach sensations immediately triggered concern.
Ironically, this kind of monitoring often intensifies the very sensations people fear. The more attention we place on internal signals, the louder those signals can become.
Part of the work therefore involved gradually shifting Jenna’s attention outward again—toward activities, environments, and everyday experiences—rather than constantly scanning for signs of danger within her body.
At the same time, we began introducing graded exposure.
This did not mean forcing Jenna into overwhelming situations. Instead, it meant carefully testing the predictions her anxiety was making.
For example, one of Jenna’s fears was leaving the house alone. Her mind predicted that if she went out without her husband, she might experience dizziness, lose control, or be unable to cope with panic. Rather than arguing with those predictions, therapy focused on gently testing them.
The first step was simply stepping outside alone for a short walk. Then walking a little farther. Then entering a shop independently. Each step was small enough to remain manageable, but meaningful enough to challenge the belief that she could not cope.
Each successful experience quietly sent a new message to her nervous system:
The body can feel uncomfortable and still be safe.
Another important part of this process involved what psychologists call interoceptive exposure—learning to tolerate bodily sensations that had previously triggered panic.
For Jenna, sensations like dizziness or nausea had become signals of danger. The immediate instinct was to escape them as quickly as possible. In the past, vomiting had sometimes served as a way to relieve the sensation temporarily.
But the relief was short-lived. And each time the behaviour occurred, it reinforced the belief that the sensation itself was intolerable.
Instead, Jenna gradually practiced allowing these sensations to rise and fall without reacting to them. She noticed the dizziness, the changes in breathing, the slight waves of nausea, and remained with them long enough to observe that they eventually passed on their own.
This was not easy at first. But over time something important began to shift. The sensations that once felt catastrophic began to feel simply uncomfortable.
And uncomfortable is very different from dangerous.
The stabilising routines introduced earlier through the TED framework also played an important role during this phase. Better sleep meant her nervous system was less reactive. Regular meals and hydration helped prevent energy fluctuations that could mimic anxiety symptoms. Daily walking continued to strengthen her confidence in movement and balance.
Together, these changes created a more stable physiological foundation against which exposure could work effectively.
Little by little, Jenna began to experience something she had not felt in months. Moments of ordinary life. A walk outside without scanning for danger. A shopping trip completed alone. An evening of sleep without waking in panic.
These were small victories, but they carried enormous meaning. Each one helped recalibrate a system that had been locked in fear. Gradually, the pendulum that once swung wildly between vigilance, avoidance, and collapse began to slow.
And with that slowing came something else Jenna had not felt in a long time: the sense that her body might once again be a place she could trust.
But the most important change was not simply the disappearance of panic.
The Moment Therapy Almost Changed Direction
Recovery from anxiety rarely follows a straight line.
For Jenna, the first months of therapy had already brought meaningful changes. The panic attacks had stopped. Vomiting episodes had reduced significantly. She was sleeping better, moving more, and gradually testing situations that had once felt impossible.
From the outside, it might have looked as though the hardest part was over.
But around the fifteenth session, something shifted.
During that week Jenna arrived at therapy noticeably distressed. The anxiety had intensified again, and the familiar sensations, dizziness, internal tension, waves of fear, felt closer to the surface than they had for several weeks. Although the panic attacks themselves had not returned, the emotional pressure she was experiencing was unmistakable.
Moments like this can be unsettling in therapy.
When symptoms reappear after progress has been made, it is easy for both therapist and client to wonder whether the improvement was temporary. The mind quickly begins asking uncomfortable questions: Is this working? Should something else be tried?
During that session we discussed the possibility of returning to her psychiatrist for a medication review. Jenna had already been taking escitalopram, and adjusting the medication was a reasonable option to consider if her distress continued to increase.
At first, the suggestion seemed as though it might signal a setback.
But something unexpected happened.
Instead of experiencing the conversation as a sign that therapy was failing, Jenna responded differently. The possibility of adjusting medication appeared to sharpen her awareness of how much progress she had already made. She realised that she did not want to retreat from the work she had been doing.
In that moment, something subtle but important shifted.
Rather than relying solely on external solutions, medication, reassurance, or avoidance, Jenna began to recognise her own role in the recovery process. The exposure exercises, the lifestyle changes, the effort to tolerate difficult sensations: these were not things being done to her. They were actions she had been taking herself.
Paradoxically, the conversation about medication strengthened her sense of responsibility and commitment.
In the sessions that followed, her engagement with the therapeutic work deepened noticeably. Exposure exercises became more consistent. She approached situations with greater confidence, even when anxiety appeared.
Instead of interpreting discomfort as a signal that something had gone wrong, she began to see it as part of the process of retraining her nervous system.
This is an important moment in many therapeutic journeys.
Recovery often accelerates when people move from seeing themselves as passive recipients of treatment to active participants in change. The focus shifts from “How do I make the anxiety disappear?” to “How do I respond differently when anxiety appears?”
For Jenna, this shift marked the beginning of a more stable phase of recovery.
The pendulum that had once swung violently between vigilance, avoidance, and collapse was slowing. The sensations that once felt catastrophic were becoming manageable.
And perhaps most importantly, the sense that her body had betrayed her was gradually being replaced by something new: a quiet but growing confidence that she could handle what her body was feeling.
Closing Reflection
Jenna’s story is not unusual. Many people who experience panic attacks assume the problem lies entirely in anxiety itself. They focus on the frightening sensations in the moment, the racing heart, the dizziness, and the feeling that something is about to go terribly wrong.
But panic often emerges at the intersection of several interacting systems: a body that has become physiologically over-reactive, an emotional system shaped by years of responsibility or vulnerability, and a mind that tries to make sense of sensations that suddenly feel unfamiliar.
When these systems fall out of balance, panic can become the language through which the nervous system signals distress. What Jenna’s journey reminds us is that recovery does not always begin where people expect. Sometimes it begins with sleep, with nourishment, and with learning to move again without fear. Sometimes it begins with understanding the patterns that quietly shaped our responses to stress long before anxiety appeared.
And sometimes, as the pendulum slows, people discover something they had not realised they had lost: the ability to trust their own body again.
For clinicians, Jenna’s case also illustrates an important point. Panic disorder can rarely be understood purely as a cognitive problem. When physiological instability, shame-based self-evaluation, and behavioural avoidance interact, treatment may need to address all three systems simultaneously.
For those experiencing panic themselves, the message is equally important.
The sensations may feel overwhelming. They may feel unpredictable. They may even feel dangerous.
But very often, they are the nervous system’s attempt to adapt.
And with the right support, the same system that once generated panic can learn something new: how to settle, how to rebalance, and how to move forward again.
This article does not aim to redefine the established understanding of panic disorder. Instead, it suggests that in some cases panic attacks may represent the final expression of earlier experiences marked by emotional neglect, which can contribute to broader regulatory imbalances involving physiological arousal, emotional signalling, and cognitive interpretation.
Traditional CBT offers well-established and effective models for the treatment of panic disorder. However, Jenna’s story illustrates how panic symptoms can sometimes emerge from earlier life experiences marked by prolonged stress, hypervigilance, and role reversal within the family. Standard CBT approaches typically focus on the maintenance of panic symptoms in the present and may explore early experiences only when they are directly linked to current beliefs or behaviours.
Contemporary CBT protocols for panic disorder commonly incorporate excellent techniques such as cognitive restructuring and interoceptive exposure, originally developed within the Panic Control Treatment model of David H. Barlow and colleagues, alongside cognitive approaches such as the catastrophic misinterpretation model proposed by David M. Clark.
Over time, however, prolonged patterns of stress and self-regulation can contribute to dysregulation across physiological, affective, and cognitive systems. Restoring balance within this body–brain–affect network can gradually transform how anxiety is experienced and regulated.
In this sense, treating panic may sometimes require more than addressing fear itself, it may require accepting a painful history and helping the body, the mind, and the emotional system learn how to work together again.
Further reading:
Barlow, D.H. (2002) Anxiety and its disorders: The nature and treatment of anxiety and panic. 2nd edn. New York: Guilford Press.
Barlow, D.H., Craske, M.G. and Meadows, E.A. (2000) ‘Mastery of your anxiety and panic: Therapist guide’, 3rd edn. New York: Oxford University Press.
Barlow, D.H., Gorman, J.M., Shear, M.K. and Woods, S.W. (2000) ‘Cognitive-behavioral therapy, imipramine, or their combination for panic disorder: A randomized controlled trial’, Journal of the American Medical Association, 283(19), pp. 2529–2536.
Barrett, L.F. (2017) ‘The theory of constructed emotion: An active inference account of interoception and categorization’, Social Cognitive and Affective Neuroscience, 12(1), pp. 1–23.
Clark, D.M. (1986) ‘A cognitive approach to panic’, Behaviour Research and Therapy, 24(4), pp. 461–470.
Clark, D.M. (1997) ‘Panic disorder and social phobia’, in Clark, D.M. and Fairburn, C.G. (eds.) Science and practice of cognitive behaviour therapy. Oxford: Oxford University Press, pp. 121–153.
Craske, M.G. and Barlow, D.H. (2007) ‘Mastery of your anxiety and panic: Therapist guide’, 4th edn. New York: Oxford University Press.
Hirsch, C.R. and Mathews, A. (2019) ‘Approaching cognitive behaviour therapy for generalized anxiety disorder from a cognitive process perspective’, Frontiers in Psychiatry, 10, p. 796.
McEwen, B.S. (2007) ‘Physiology and neurobiology of stress and adaptation: Central role of the brain’, Physiological Reviews, 87(3), pp. 873–904.
Mirea, D. (2025) The transdiagnostic application of NeuroAffective-CBT®: A case study of chronic stress and burnout. Available at: https://neuroaffectivecbt.com (Accessed: March 2026).
National Institute for Health and Care Excellence (2020) Generalised anxiety disorder and panic disorder in adults: Management (CG113). London: NICE.
Confidentiality note: Jenna is a composite clinical vignette based on several cases. Identifying details have been altered to protect confidentiality.
NeuroAffective Narrative Reconsolidation (NNR) is a trauma-processing method developed within the NeuroAffective-CBT (NA-CBT) framework. The approach integrates principles from trauma-focused cognitive behavioural therapy, affective neuroscience, and dual-attention trauma processing to enable clients to revisit traumatic memories while maintaining physiological regulation and present-moment awareness.
Unlike interventions that focus primarily on cognitive restructuring, NNR emphasises the coordinated engagement of physiological regulation, affective processing, and narrative meaning-making. The model assumes that traumatic memories often persist because they remain encoded as ongoing threat experiences rather than integrated autobiographical events.
The central therapeutic objective of NNR is the development of what NA-CBT conceptualises as the Integrated-Self, a state in which traumatic experiences can be recalled without triggering overwhelming emotional or physiological responses. Through structured cycles of narrative activation, somatic tracking, distress modulation, and identity integration, the intervention aims to facilitate memory reconsolidation and transform trauma memories into coherent elements of personal narrative.
This article outlines the theoretical foundations of NNR and situates the method within the broader NA-CBT treatment framework. A detailed clinical case illustration then demonstrates how trauma memories may gradually shift from overwhelming threat experiences toward integrated life events, supporting the emergence of a more stable and resilient sense of self. The clinical implications of this approach and its relevance for future research on trauma integration and memory reconsolidation are also discussed.
Cognitive-Behavioural Therapy (CBT) remains one of the most empirically supported psychological treatments across a wide range of mental health disorders. Its strength lies in its structured, transparent, and collaborative focus on the relationships between thoughts, behaviours, and emotional responses. Yet over the past two decades, developments in neuroscience and trauma psychology have increasingly highlighted something clinicians have long observed in practice: emotional suffering cannot be fully explained, or resolved, through cognition alone.
Trauma illustrates this limitation particularly clearly. Clients frequently report that they intellectually understand that the event is over, yet their bodies continue to react as if the threat were still present. Their heart rate accelerates, their stomach tightens, breathing becomes shallow, and muscles brace defensively, sometimes before a conscious thought has formed. Insight may be present, yet the nervous system remains unconvinced.
NeuroAffective-CBT was developed in response to this clinical reality. The model represents an integrative therapeutic framework that combines insights from affective neuroscience, physiological regulation, and cognitive-behavioural therapy into a unified approach to emotional distress. Within NA-CBT, psychological suffering is conceptualised as emerging from dysregulation within a body–brain–affect system, in which physiological arousal, emotional experience, and cognitive interpretation continuously interact.
From this perspective, the brain functions fundamentally as a predictive organ. Its primary task is not abstract reasoning but survival. It constantly evaluates whether the organism is safe. When physiological signals, such as increased heart rate, muscle tension, pain, or breathlessness, indicate possible danger, the brain rapidly amplifies threat interpretations. These interpretations reinforce anxiety, avoidance, hypervigilance, and negative beliefs about the self or the world. Over time, this cycle may become self-perpetuating.
Therapeutic change therefore cannot rely solely on cognitive restructuring. If the body continues to generate threat signals, cognition is placed in a reactive position, attempting to reason with an alarm that has already been activated. Sustainable recovery requires coordinated regulation of physiology, affect, and cognition. It involves helping the nervous system experience safety while traumatic memories are revisited.
Integration Within NA-CBT
NeuroAffective-CBT synthesises several theoretical influences into a coherent clinical framework. Rather than treating cognition, emotion, and physiology as separate domains, the model conceptualises them as interacting components of a single regulatory system. This perspective is captured in what NA-CBT describes as the Body–Brain–Affect model (Figure 1), a central conceptual element that illustrates how emotional experience emerges through the continuous interaction between physiological signals, emotional states, and cognitive interpretation.
Within this framework, physiological signals from the body influence emotional states, which in turn shape cognitive interpretations of threat and safety. When the body signals danger through pain, tension, or heightened arousal, the brain rapidly generates emotional responses that influence perception and thought. Conversely, cognitive interpretations may amplify or soothe emotional responses, which subsequently feed back into physiological regulation.
From a therapeutic perspective, this triangle highlights an essential principle: effective treatment must address all three domains simultaneously. Improvements in physiological regulation often reduce emotional reactivity, making cognitive updating more accessible. Changes in cognitive interpretation may soften emotional responses and allow the body to relax. Likewise, emotional processing occurring within a safe relational context may enable both physiological and cognitive systems to reorganise.
Within NA-CBT, this integrated understanding forms the conceptual foundation upon which later treatment modules, including trauma processing through the NeuroAffective Narrative Reconsolidation (NNR) protocol, are built.
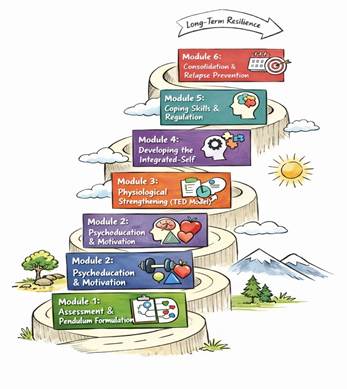
Treatment Structure of NeuroAffective-CBT
NA-CBT is delivered through six sequential treatment modules designed to progressively stabilise physiological regulation, before processing traumatic experiences, in order to consolidate long-term psychological resilience. Each module builds upon the previous phase, moving from assessment and stabilisation toward trauma integration and relapse prevention (Figure 2).
Module 1: Assessment and the Pendulum-Effect Formulation Comprehensive clinical assessment focusing on predisposing, precipitating, perpetuating, and protective factors. Development of the NA-CBT pendulum formulation mapping oscillations between three main self-sabotaging strategies: avoidance, overcompensation, and capitulation (in no particular order).
Module 2: Psychoeducation and Motivation Introduction to the Body–Brain–Affect model and the pendulum-effect framework. Psychoeducation about physiological regulation, trauma responses, and the interaction between cognition, affect, and bodily states.
Module 3: Physiological Strengthening (TED Model) Stabilisation of biological rhythms through the TED (Tired-exercise-Diet) model, emphasising sleep regulation, physical activity, and nutritional stability as foundations for emotional regulation. TED can be expanded to work with various conditions.
Module 4: Developing the Integrated-Self Trauma processing through the NeuroAffective Narrative Reconsolidation (NNR) protocol, integrating narrative activation, somatic tracking, distress modulation, and identity reconstruction.
Module 5: Coping Skills Development and generalisation of adaptive coping strategies and cognitive-behavioural skills to support resilience in everyday situations.
Module 6: Consolidation and Relapse Prevention Integration of therapeutic gains, future-oriented planning, and relapse prevention strategies to maintain long-term emotional stability.
NeuroAffective-CBT: Theoretical Foundations
The theoretical foundations of NeuroAffective-CBT draw upon several complementary areas of psychological and neuroscientific research. Rather than positioning itself as a replacement for cognitive-behavioural therapy, NA-CBT extends the traditional model by integrating insights from attachment theory, affective neuroscience, trauma memory research, and identity psychology.
These perspectives converge around a central clinical observation: emotional suffering rarely arises from cognition alone. Instead, it emerges through the interaction between biological regulation, emotional processing, and personal meaning.
Trauma may be understood, at its most fundamental level, as an adaptive alert system. When an individual experiences or witnesses a life-threatening situation, the brain, whose primary function is survival, encodes the event in ways that allow future detection of similar danger. From that point onward, the nervous system becomes sensitised to cues associated with the original threat, generating anticipatory anxiety and protective vigilance aimed at preventing further harm.
Under most circumstances, this mechanism serves an adaptive purpose. However, post-traumatic stress symptoms may develop when autobiographical memory becomes disorganised and the individual’s interpretation of the event shifts toward a pervasive sense of vulnerability or incapacity (e.g., I cannot cope with similar threats). In such cases, the trauma narrative may contribute to a destabilised sense of identity, often expressed as a feeling that “I am no longer the person I used to be”.
Importantly, not every individual exposed to a frightening event develops trauma-related symptoms. Vulnerability to post-traumatic stress is influenced by multiple factors, including early developmental experiences, pre-existing cognitive schemas, attachment patterns, and available social support. Nevertheless, the capacity to generate fear responses to predicted danger is deeply embedded within mammalian neurobiology. The difference between adaptive fear and persistent trauma lies in how the experience becomes encoded, interpreted, and integrated within the individual’s broader autobiographical narrative.
Within this broader framework, specific therapeutic procedures are required to translate these principles into clinical practice. It is within this theoretical context that the NeuroAffective Narrative Reconsolidation (NNR) protocol emerges as a clinical method for trauma processing.
Attachment, Development, and Coping Patterns
From the perspective of NA-CBT, the brain’s primary survival functions begin long before conscious reasoning develops. Early relational experiences shape how the nervous system learns to detect safety and danger. Attachment theory has long helped psychotherapists understand patterns of emotional regulation, dependency, avoidance, and relational security.
Within NA-CBT, attachment styles are understood as patterns emerging from the interaction between the child’s developing neurobiology and the caregiving environment. Early experiences of emotional attunement, neglect, predictability, or threat become encoded not only as autobiographical memories but also as physiological patterns of emotional regulation.
Children raised in predictable and responsive environments typically develop nervous systems that expect safety and connection. Conversely, environments characterised by emotional neglect, inconsistent care, or exposure to threat may shape nervous systems that become chronically vigilant, avoidant, or defensive.
For this reason, developmental history plays a meaningful role in the assessment phase of NA-CBT. Childhood narratives are explored not for their own sake, but because they often illuminate how individuals learned to regulate emotion, seek support, or defend themselves psychologically.
In clinical practice, assessment therefore becomes a collaborative process of guided discovery rather than a mechanical checklist. Therapists listen for several interacting domains that help organise the client’s story: predisposing factors, precipitating events, perpetuating mechanisms, and protective factors. Understanding these domains allows clinicians to appreciate not only what has contributed to distress but also what strengths remain available within the client’s life narrative.
Affective Neuroscience
Insights from affective neuroscience further clarify why cognitive insight alone is often insufficient to resolve trauma-related distress. Emotional responses frequently originate in subcortical threat-detection systems that operate rapidly and automatically, often before conscious cognitive appraisal occurs (LeDoux, 2015). These neural systems evolved to prioritise survival and are therefore highly sensitive to signals of danger.
As a result, trauma memories are rarely encoded as purely verbal or conceptual experiences. Instead, they are often stored as multisensory experiences involving bodily sensations, emotional states, and perceptual fragments. A racing heart, tightening stomach, or sudden surge of fear may therefore occur even when the individual rationally understands that the present moment is safe.
Recognising this helps explain why therapeutic approaches that incorporate physiological awareness and regulation often prove more effective in trauma work than those relying solely on cognitive dialogue.
Trauma Memory Models
The cognitive model of post-traumatic stress disorder proposed by Ehlers and Clark (2000) provides another important theoretical foundation for NA-CBT. According to this model, trauma symptoms persist when memories of the event remain insufficiently integrated within autobiographical memory.
Rather than being recognised as events that occurred in the past, trauma memories are experienced as ongoing threats in the present.
In practice, this means that reminders of the trauma, sounds, bodily sensations, environments, or thoughts, can reactivate the original threat response. Individuals may experience intrusive recollections, flashbacks, or intense emotional reactions that feel immediate and overwhelming.
From a NeuroAffective perspective, these responses reflect the nervous system’s difficulty distinguishing between memory and present danger.
Shame and Self-Identity
Traumatic experiences frequently influence identity as much as emotional regulation. Research on shame and vulnerability demonstrates how adverse experiences can reshape the narratives individuals hold about themselves (Brown, 2012). Traumatic events are not only remembered as external occurrences but are often internalised as reflections of personal inadequacy or vulnerability.
A traumatic event may give rise to beliefs such as I am weak, I am permanently damaged, I am ashamed of what happened, or I cannot trust the world. These identity-based interpretations may become deeply embedded, shaping behaviour, expectations, and interpersonal relationships long after the original event has passed.
Within the NA-CBT framework, attention to identity narratives therefore becomes an essential component of trauma recovery. Therapeutic work involves not only reducing fear responses but also helping clients reconstruct a coherent and compassionate understanding of themselves.
Addressing internalised shame is particularly important in this process. Shame can be understood as a socially mediated form of threat response, involving fears of rejection, exclusion, or negative evaluation by others. It is frequently associated with beliefs about being fundamentally flawed, socially rejected, or unworthy of acceptance. When such beliefs remain unexamined, they may perpetuate avoidance, withdrawal, and emotional dysregulation. Bringing these shame-based narratives into conscious awareness within the safety of a supportive therapeutic context, allows them to be re-evaluated and integrated, thereby supporting both emotional regulation and identity reconstruction.
Memory Reconsolidation
Neuroscience research on memory reconsolidation provides an additional explanatory framework for therapeutic change. Traumatic experiences are often encoded under conditions of intense emotional arousal, which can disrupt the normal integration of sensory, emotional, and contextual information. As a result, trauma memories may be stored in fragmented or poorly integrated forms, contributing to disorganised recollection and intrusive re-experiencing.
Research suggests that when emotional memories are reactivated under conditions of relative safety, they temporarily enter a labile state in which they can be modified before being stored again, a process referred to as memory reconsolidation (Lane et al., 2015; Nader and Hardt, 2009). During this window, new emotional or contextual information may become incorporated into the existing memory trace.
Within therapy, revisiting traumatic memories in a regulated and supportive context may therefore allow the nervous system to encode new emotional associations alongside the original experience. The event remains remembered, but its emotional intensity and subjective meaning may gradually change.
Dual-Attention Processing
Traumatic experiences are frequently encoded under conditions of extreme threat, during which heightened physiological arousal and stress hormones can narrow attentional focus toward the perceived source of danger. As a result, individuals often recall highly salient threat-related details while other contextual information remains poorly encoded. For example, victims of violent assault may vividly remember the weapon involved while recalling relatively few details about the surrounding environment.
Trauma therapies such as Eye Movement Desensitisation and Reprocessing (EMDR) emphasise the importance of maintaining simultaneous awareness of the traumatic memory and present-moment safety. This process, often described as dual-attention, allows individuals to revisit distressing memories while remaining oriented to the current environment and the therapeutic relationship (Shapiro, 2018).
Maintaining this broader attentional field may help prevent full re-immersion in the traumatic experience. Instead, the memory is held within a wider context that includes bodily regulation, environmental orientation, and cognitive reflection. This expanded awareness may support the integration of previously inaccessible contextual information, allowing fragmented memories to be reorganised into a more coherent autobiographical narrative.
Core Principles of NeuroAffective Narrative Reconsolidation (NNR)
NeuroAffective Narrative Reconsolidation (NNR) is guided by several core therapeutic principles derived from cognitive-behavioural trauma models, affective neuroscience, and memory reconsolidation research. First, traumatic memories must be sufficiently activated for the underlying memory network to become accessible for modification. Second, this activation must occur under conditions of physiological regulation and interpersonal safety, allowing the nervous system to remain within a tolerable window of emotional engagement. Third, therapeutic change occurs when new contextual, emotional, and cognitive information becomes integrated into the reactivated memory trace.
Within NA-CBT, this process is supported through the coordinated engagement of narrative activation, somatic awareness, distress modulation, and identity reconstruction. Rather than focusing exclusively on cognitive reinterpretation, the NNR protocol emphasises the simultaneous regulation of physiological arousal, emotional processing, and autobiographical meaning. Through repeated cycles of regulated memory activation and updating, traumatic experiences can gradually shift from present-tense threat states toward integrated autobiographical memories.
NeuroAffective Narrative Reconsolidation and the Integrated-Self
It is within this theoretical context that the NeuroAffective Narrative Reconsolidation (NNR) protocol was developed. NNR represents the primary trauma-processing intervention used in Module 4 (out of 6) of NA-CBT, the module referred to as Developing the Integrated-Self.
The aim of NNR extends beyond simple symptom reduction. Its deeper objective is integration. Within NA-CBT, the Integrated-Self refers to a psychological state in which traumatic experiences are incorporated into autobiographical narrative rather than experienced as ongoing threats. The memory remains accessible, but it no longer carries the same physiological urgency or identity-disrupting meaning. The individual can look back without being pulled back into the emotional state of the original event.
NNR draws upon several established therapeutic mechanisms. From trauma-focused CBT it incorporates imaginal reliving, hotspot identification, and cognitive updating. From EMDR-informed approaches it adopts the principle of targeted memory activation combined with dual attention, maintaining awareness of both the traumatic memory and present-moment safety. From affective neuroscience it integrates interoceptive awareness and autonomic regulation.
What distinguishes NNR is the deliberate sequencing and simultaneous engagement of these processes within a coherent and relationally grounded therapeutic framework.
This article presents NNR through a clinical case illustration. Rather than outlining the protocol in purely procedural terms, the case demonstrates how the method unfolds in practice: how physiological stabilisation prepares the ground for memory activation, how distress modulation creates the conditions for reconsolidation, and how identity integration transforms the meaning of trauma without denying its reality.
The case illustration presented later in the article demonstrates how the Integrated-Self may emerge through a carefully guided reconnection between body, affect, and autobiographical narrative.
Why the Integrated-Self Matters
Following trauma, many individuals report not only fear-related symptoms but also a disruption in their sense of identity continuity. They often describe an internal division between the person I was before and the person I am now. Even when external functioning appears intact, the trauma may persist internally as an unintegrated chapter that intrudes into the present through physiological surges, intrusive imagery, avoidance patterns, and shifts in self-appraisal.
From an NA-CBT perspective, this represents not merely a problem of memory content but of memory status. A trauma memory that remains “threat-coded” functions like an alarm in the present rather than a narrative of the past. The individual may be able to describe the event factually, yet the nervous system responds as though the danger is occurring again. This disrupts meaning-making, reduces agency, and often reshapes identity through interpretations such as I am unsafe, I am weak, or I cannot trust my body.
Within NA-CBT, the Integrated-Self refers to the stage at which traumatic experiences can be recalled without triggering a present-tense threat response. The event is neither erased nor minimised. Instead, it becomes located appropriately in time and meaning, an autobiographical memory rather than a re-lived danger state. The individual can look back without being pulled back into the emotional state of the original event.
Accordingly, the therapeutic aim is not to eliminatememory but to achieve integration: restoring continuity of self, updating meaning, and enabling the nervous system to learn, through experience rather than instruction, that the present is no longer the past.
A NNR Protocol for Trauma Processing
When clinicians and clients speak about “processing trauma”, it is often imagined as a primarily cognitive task: challenging beliefs, reframing interpretations, or practising coping statements. In clinical reality, however, trauma is rarely represented only in language. It is frequently expressed first through physiology, tightness in the chest, visceral constriction, trembling, heat surges, bracing muscles, and rapid shifts in breathing, often occurring before explicit meaning is consciously formed. Cognition then attempts to make sense of a state the nervous system has already entered: “I am not safe”.
NeuroAffective-CBT was developed with this premise at its core. The model assumes that post-traumatic distress is not a single-system phenomenon but an ongoing interaction between social context, physiology, affect, and cognition, each shaping the others in real time. Humans are fundamentally social organisms, and the relational environment in which trauma is revisited therefore plays a crucial therapeutic role. Particular attention is given to the authenticity and safety of the relationship between therapist and client. Clinical experience and psychotherapy research suggest that outcomes are strengthened when clients experience the therapist as both professionally competent and interpersonally safe, particularly in trauma work where shame and threat sensitivity may be elevated. Within a safe therapeutic relationship, clients are often better able to confront painful memories while reducing the shame and self-judgement that frequently accompany traumatic experiences.
If trauma is encoded and maintained across social, physiological, affective, and cognitive systems, recovery must engage these systems together, coordinating bodily regulation, affect tolerance, and narrative meaning-making within a single therapeutic process.
Within Module 4 of NA-CBT (Developing the Integrated-Self), this coordinated process is operationalised through NeuroAffective Narrative Reconsolidation. NNR is not a simple combination of CBT and EMDR techniques, nor a rebranding of existing trauma protocols. Rather, it is a structured method for integrating traumatic memories into autobiographical narrative while maintaining sufficient regulation to allow updating and reconsolidation to occur without overwhelming the client.
The sections below clarify why the concept of the Integrated-Self is clinically relevant and outline the mechanistic logic that informs the NNR protocol.
The Rationale of NeuroAffective Narrative Reconsolidation
NNR is guided by a principle shared across cognitive and neurobiological trauma models: when a memory is reactivated under conditions of safety, it becomes available for updating. Trauma processing therefore requires more than recall; it requires recall paired with regulation and new information.
In cognitive-behavioural terms, this includes imaginal reliving, hotspot identification, cognitive updating, and meaning reconstruction. In EMDR-informed terms, it echoes the principle of dual attention: the capacity to keep one “foot” in the memory while maintaining connection to the present environment and the therapeutic relationship. In NA-CBT terms, it is a body–affect–meaning integration process: the therapist tracks how the body responds, supports affect tolerance, and facilitates narrative updating in ways that are congruent with physiological state.
The distinctive contribution of NNR is not any single element. It is the deliberate sequencing and simultaneous engagement of core mechanisms, narrative activation, somatic tracking, distress modulation, perspective shifting, identity reframing, and future orientation, within a coherent arc designed to support reconsolidation rather than retraumatisation.
NNR assumes that effective trauma processing requires three conditions:
Sufficient activation of the target memory (so the network is accessible for modification).
Sufficient regulation (so activation remains within a tolerable window and does not collapse into overwhelm or dissociation).
Sufficient updating information (so the memory can be re-encoded with new context, meaning, and embodied safety).
Within NA-CBT, Modules 1–3 (see treatment pathway above) function as preparation for this work by strengthening regulation capacity and stabilising the threat–safety pendulum. NNR is then introduced when the client can reliably engage regulation strategies and remain oriented to the present while recalling distressing material.
Overview of the NNR Clinical Sequence
Although adapted to individual presentation, NNR typically follows a replicable structure:
Narrative activation of the event in present-tense or vivid recall.
Somatic tracking of physiological shifts and localisation of distress.
Hot memory selection to target the most emotionally loaded moment.
Distress modulation using breathing, grounding, and imagery (e.g., dial/clock reduction) to bring arousal into a tolerable range.
Cognitive updating by incorporating new interpretations, information, or corrective emotional experience.
Identity reframing linking the event to resilience-based self-meaning (without denial of harm).
Values and meaning integration, where relevant, to stabilise new schemas.
Future orientation and relapse planning to consolidate learning and reduce avoidance.
This structure ensures that memory activation is not merely endured but actively transformed, experienced within a context of regulation, updated meaning, and a revised identity narrative consistent with psychological integration.
Rationale for the Case Illustration
The remainder of this article illustrates the NNR protocol through a clinical case example. Rather than presenting the method solely in procedural terms, the case demonstrates how the intervention unfolds moment-to-moment in practice. In particular, it illustrates how physiological stabilisation prepares the ground for memory activation, how distress modulation supports tolerable engagement with traumatic material, and how identity integration can transform the meaning of trauma without denying the reality of the event.
The case that follows illustrates how the Integrated-Self can emerge through a carefully guided reconnection between body, affect, and autobiographical narrative.
A case illustration: “Edward”
“Edward” (pseudonym) was a physically active 19-year-old man who presented with persistent trauma symptoms following a severe abdominal injury sustained during a boxing sparring session. The injury led to emergency hospital treatment and surgical removal of his spleen. In the months that followed he experienced intrusive recollections, anxiety around medical environments, avoidance of contact sport, reduced confidence, and a sense that his future had narrowed. His identity, previously anchored in physical competence and sport, felt disrupted, as though his body had become unfamiliar territory.
During the initial sessions of NA-CBT, the therapeutic focus was on preparation. This included developing a collaborative therapeutic relationship, establishing a shared formulation (the pendulum-effect), and mapping maintenance patterns. A particularly important aspect of this phase involves preparing the client for trauma processing by fostering realistic hope and an optimistic treatment expectancy. This is supported through the use of metaphors and evidence-informed psychoeducation concerning trauma memory processing, stress hormones, brain function, and emotional regulation. Practising and strengthening physiological and emotional regulation capacities prior to NNR is considered an essential prerequisite for trauma processing. Without such preparatory work, trauma processing may lead to excessive activation without sufficient containment, potentially leaving the client more overwhelmed than before therapy began.
By the time we entered Module 4, Edward had established a trusting bond with the therapist and could already recognise how his vulnerability, the sense of being weaker, more exposed, less “himself”, was perpetuated by what NA-CBT calls the Pendulum-effect (formulation). He oscillated between three coping modes. There was overcompensation: keeping constantly busy so his mind didn’t return to the event, working hard and filling time to outrun memory. There was hypervigilant avoidance: scanning for danger, steering away from reminders, refusing situations where he might feel physically threatened, even avoiding looking at or touching the scar. And there was capitulation: collapsing into self-criticism and shame when he noticed he had withdrawn again, telling himself he was “weak” for struggling.
From a therapeutic perspective, the autobiographical split was immediately apparent: what I am now is not who I was. And while the self-sabotaging patterns were predictable, they did not feel chosen. They felt automatic, rather than a set of strategies he was consciously selecting.
This is precisely where Integrated-Self work begins: stabilising the pendulum enough that the client can look back without being pulled under.
Disclaimer: Details of individual cases have been modified to protect confidentiality while preserving the clinical process described.
The NNR session: opening the memory, keeping the body safe
When trauma processing began, Edward was invited to recount the event as if it were occurring in the present moment. Gentle prompts such as, “What happens next?” were used to help maintain the client’s attention on the unfolding timeline while supporting a sense of safety and continuity. This process is important in reducing gaps or fragmentation in the trauma narrative before broader contextualisation and perspective shifting are introduced. Only once the memory sequence has been sufficiently elaborated can alternative perspectives and updated meanings be explored without prematurely disrupting the integrity of the original memory representation.
The use of present-tense narrative, as much as possible, was therefore intentional. Trauma memories are not typically stored as structured verbal narratives but rather as multisensory experiences involving bodily sensations, emotions, and perceptual fragments. Present-tense recall helps reactivate the memory network in a way that resembles its original encoding, thereby making it accessible for therapeutic updating.
As Edward narrated the event, attention was repeatedly redirected toward bodily sensations. He was asked to notice where distress appeared in his body, what sensations changed, and how his physiological state shifted as the memory unfolded. Where does he feel it? What changes? What tightens? What heats? What collapses? The distress was primarily located in the central body, where the surgery scar was also located, manifesting as strong tension at the front of the upper torso, concentrated around the scar area. Edward was asked to rate the distress on a 0–10 scale, in order to track the intensity of the physiological response and to also establish a shared language for tracking regulation and change, observing shifts in emotional activation throughout the session, rather than becoming lost inside them.
Two highly distressing “hot memories” emerged quickly. One was the moment he was punched in the abdomen. The other was later, in hospital, when he was told that his spleen would need to be surgically removed. Both were highly activating: the hospital memory reached 10/10, while the punching memory was rated slightly lower at 9.5/10.
At this point an important clinical step occurred. Edward was invited to choose which memory he wished to process first, the one that felt most pressing or manageable to approach in the current session. He selected the hospital moment.
This choice was clinically significant. Trauma frequently involves experiences of helplessness or loss of control; inviting the client to select the focus of processing helps restore a sense of agency precisely where trauma had removed it.
Dialling Down Distress: Clock Imagery and Physiological Regulation
Before further processing, the focus shifted toward physiological regulation. Grounding breathwork, progressive muscle relaxation, and body-scanning exercises were introduced, followed by an imagery technique commonly used within NA-CBT trauma work: clock-dial imagery (see Figure 3).
Distress modulation is normally facilitated through a guided imagery technique referred to in NA-CBT as NeuroAffective Distress Modulation, also described as the clock-dial regulation method. The technique invites clients to imagine gradually reducing physiological arousal by “turning down” an internal dial while synchronising the imagery with slow exhalation and bodily relaxation.
The idea is simple yet clinically effective. With each slow exhalation, the client imagines turning a dial downward, from 10 to 9, from 9 to 8, and progressively lower, until the level of distress reaches 5 or below. In early sessions, it may be unrealistic to expect distress to fall substantially below SUD 5, particularly when the target memory is highly activating. The reduction in distress is guided by the natural rhythm of breathing and gradual physiological settling.
Figure 3 describes the NeuroAffective Distress Modulation or Clock-Dial Technique: a guided imagery method in which clients synchronise slow exhalation with an imagined reduction in distress (e.g., from SUD 10 toward SUD 5). Gentle hand movements may be used to embody the “dialling down” action while maintaining relaxed posture and minimal muscular effort.
During this process, Edward was encouraged to imagine physically turning the dial with his hands and/or outbreath. In some cases, the imagery may be paired with gentle physical movement: clients raise their hands slightly during inhalation and, during exhalation, allow the hands to lower naturally as if turning the dial downward, gradually reducing the intensity of distress with each out-breath. If physical movement is introduced, it is important that it remains relaxed and free of muscular strain, and that it does not distract from the primary purpose of the exercise, facilitating physiological regulation and emotional settling.
This imagery serves a specific therapeutic function. It provides traumatised individuals with a felt sense of influence over emotional intensity. Clients sometimes describe this experience as gaining “control,” but the therapeutic aim is more accurately described as restoringagency rather than suppressing emotional responses. In this sense, the imagery functions as a bridge between cognitive intention and bodily regulation, an internal interface through which the client can actively modulate physiological arousal.
As Edward practised the technique, his distress gradually reduced to approximately SUD 5 (SUDS; 0-10). The decision to pause at this level was deliberate. The aim was not to eliminate emotional activation but to maintain it within a tolerable window of engagement, where emotional processing and cognitive updating could occur without overwhelming the client.
Importantly, subjective distress ratings do not always correspond precisely with observable physiological responses. For this reason, the therapist also monitored behavioural and physiological cues such as breathing patterns, muscular tension, and posture. At one point, for example, the therapist noted persistent tension in Edward’s shoulders and continued constriction in his breathing. Edward was therefore gently invited to re-evaluate his distress rating: “I notice your shoulders are still quite tense and your breathing appears somewhat restricted. Are you sure the level has come down to five? If not, that is completely normal… we can take another moment and continue the exercise”.
Such moments of collaborative checking help ensure that regulation reflects genuine physiological settling rather than a cognitive attempt to “perform well” in therapy.
At this stage, the NNR protocol shares certain conceptual similarities with trauma-processing principles used in EMDR. Rather than maintaining narrow attentional focus on the traumatic image, the intervention deliberately expands awareness. Edward remained connected to the memory while simultaneously anchoring his attention in his breathing, bodily sensations, and the present therapeutic environment.
This broader attentional field allowed the nervous system to begin learning a crucial distinction: the memory was being recalled, but the threat itself was no longer present.
The imagery used during this phase of processing serves two primary functions. First, it should help reduce physiological arousal by activating calming imagery that signals safety to the body–brain–affect system. Second, it should be meaningful to the individual client. Imagery is therefore tailored to the client’s personal preferences, cultural background, and sources of relaxation or comfort.
Research on mental imagery in psychotherapy suggests that individuals can generate vivid internal scenes that promote emotional regulation and self-soothing (Hackmann, Bennett-Levy and Holmes, 2011). These images often engage multiple sensory modalities and may involve colours, sounds, smells, bodily sensations, or environmental scenes associated with safety and calm. Activating such multisensory representations may facilitate parasympathetic regulation and the release of endogenous opioids such as endorphins, contributing to subjective feelings of relaxation.
Assessing protective factors early in therapy can therefore provide therapists with valuable cues for identifying imagery that may support regulation and resilience during trauma processing.
Shifting Perspective: Widening the Narrative Context
Once distress had reduced to a manageable level, Edward was invited to revisit the hospital scene from an observer perspective. To support this process, we briefly located the hospital using Google Street View. The purpose was not to intensify exposure, but to help the brain anchor the memory within a concrete, real-world context, a place that exists in the external world, rather than an internal space repeatedly reactivated by flashbacks.
This step is not intended as a distraction, nor as an attempt to impose forced positivity. Rather, it functions to widen attentional focus, allowing the brain to encode contextual information that may not have been accessible during the original traumatic experience. Under conditions of acute fear, perception tends to narrow significantly as attention becomes focused on the immediate source of threat. As emotional arousal decreases, cognitive and perceptual fields can expand, allowing previously unnoticed elements of the situation to be recalled.
Edward was therefore asked to consider whether additional details could be remembered from the scene. Were there moments of reassurance? Was there evidence of professional competence or supportive presence, perhaps a nurse, a doctor, or a brief interaction that conveyed safety or care?
What gradually emerged was not a denial of the frightening nature of the event but a broader contextual understanding. Alongside fear and vulnerability, the memory also contained elements of medical competence, support, and human presence. These details are clinically important because they function as corrective contextual information. They allow the meaning of the memory to shift from “I was powerless and alone” toward a more integrated narrative: “I was terrified, and I was also cared for, treated, and ultimately survived”.
This process represents cognitive updating, but it is not purely intellectual. As the narrative context expands, emotional responses often shift as well. Clients frequently report subtle changes in bodily tension, breathing, or overall affect as the story becomes less narrowly defined by threat and more integrated within a broader autobiographical framework.
The “Warrior Scar” and Tattoo Message: Symbols of Safety, Identity Integration, and Meaning
Edward carried shame about his scar and what the injury appeared to imply about him. Within the Integrated-Self module, this is precisely the type of meaning targeted for therapeutic updating: not only the memory of what occurred, but the narrative the client has come to attach to it.
We therefore explored an alternative narrative: the scar as a battle scar, a “warrior scar”, not a symbol of defectiveness, but evidence of survival. This was not introduced as a slogan, but as an invitation: if the scar could speak, what might it say? Knowing that Edward was a martial arts enthusiast, we used a culturally congruent metaphor: what might a Samurai warrior say about visible scars earned in battle? Within that frame, scars are often interpreted not as signs of weakness but as symbols of endurance, resilience, and continued capacity.
Edward was asked what he had learned or gained, however unwillingly, from the experience and what message he now carried forward. His response emerged with notable clarity: I survived. I’m wiser. I’m smarter now through this experience. I feel closer to my parents. Closer to God. I appreciate life more. This moment represented more than simple reframing. It reflected integration, trauma being woven into identity without being allowed to define identity.
Such shifts rarely emerge spontaneously. More often, they are quietly prepared during earlier stages of therapy, frequently during the assessment phase, long before formal trauma processing begins.
The NA-CBT assessment stage is sometimes misunderstood as merely structured information gathering. In practice, it resembles a compassionate journey of guided discovery through the client’s life narrative. The therapist listens not only for predisposing factors, precipitating triggers, and perpetuating maintenance loops, but also, crucially, for protective factors: aspects of the individual that continue to point toward safety, connection, meaning, and agency.
This process requires genuine curiosity, not intrusive curiosity, but a steady and respectful interest in the client as a whole person rather than a bundle of symptoms. Many clinicians naturally attend to the most visible protective factors: supportive parents, partners, or close friends. These are important. Yet some of the most powerful protective factors are quieter and more symbolic, and they may easily be overlooked unless the therapist is actively attentive to them. A hobby. A sport. A personal value system. A creative outlet. A spiritual anchor. A life motto. A piece of art. A tattoo.
A subtle protective factor emerged in Edward’s assessment in precisely this way. A tattoo became visible beneath his sleeve, and when I asked about it, he described the courage he drew from a personal quote inked on his arm:
“For God has not given us a spirit of fear, but of power and of love and of self-discipline and self-control.”
Within the NNR protocol, such values are treated as identity anchors, not as beliefs imposed by therapy, but as the client’s own language of resilience and agency. The quote was revisited during processing, not as religious counselling, but as a personal resource. It helped challenge the trauma-belief cluster often associated with shame, “I am useless, weak, and vulnerable”, and supported the development of a more coherent organising belief: fear is a state, not an identity. Fear may surge, the body may react, and intrusive memories may arise; yet none of these experiences need define the self.
From a clinical perspective, what is occurring here is not simply positive thinking. Rather, it involves the deliberate recruitment of protective factors into conscious awareness, enabling them to be accessed reliably under conditions of stress. When trauma pushes individuals into survival modes, avoidance, overcompensation, or collapse, protective factors may feel distant or irrelevant. The Integrated-Self module restores access to these resources by incorporating them directly into the reconsolidation process itself. In other words, therapists do not wait until trauma processing is complete to remind the client who they are. Instead, the self is brought into the processing so that the memory is updated in the presence of agency, meaning, and safety.
This principle extends beyond Edward’s case and becomes particularly evident in grief-related trauma. In one bereavement case (details anonymised), a client discovered that his fiancée had died from an overdose and found her body in their garden, seated on a swing. The shock of that moment became a recurring flashback and “hot memory”, not only visually distressing but also morally and existentially destabilising.
Over time, the client began to draw an image that captured his grief: a young woman seated on a swing, her posture heavy and resting, suspended within a quiet, dreamlike landscape (Figure 4 – a symbolic swing scene later modified by the addition of an eye representing continuing bond, hope, and future-oriented meaning). During assessment and subsequent therapeutic processing, the drawing was explored not only as an expression of sorrow but also as a doorway into meaning. The client later added an open eye symbol beneath the scene, his own symbolic gesture suggesting that she remained present in some form, watching over him, and that she would want him to continue living rather than disappearing into endless mourning.
The addition of the eye did not remove grief; rather, it altered the client’s relationship to grief by introducing a sense of continuing bond, care, and permission to move forward.
This example illustrates why NA-CBT places strong emphasis on protective factors, even subtle ones, during assessment and throughout Module 4. A tattoo, a drawing, a hobby, a sport, or a newly discovered passion during recovery should not be dismissed as peripheral elements. Such elements can function as NeuroAffective safety cues, anchoring attention and supporting identity integration precisely at the moment when trauma threatens to collapse the self into fear and shame.
When trauma processing achieves integration, the observable signs are often subtle rather than dramatic. Toward the end of an NNR session, a gentle clinical check question may be used: “If you look back now at the worst moment we discussed, how clear does it feel? Does it still feel as though it happened yesterday?” Clients are reassured that after successful processing, memories may feel somewhat foggier, more distant, or less emotionally vivid. This shift can initially provoke concern: “Am I forgetting?” Yet it often reflects precisely the outcome therapy aims to achieve. The memory remains accessible, but it no longer intrudes into the present with the same emotional urgency.
When Edward later reported that the hospital moment felt more distant and less vivid, accompanied by a substantial reduction in emotional intensity, the change did not represent erasure of the event. Rather, it reflected memory reconsolidation in lived form.
What Is Happening Beneath the Surface
If the NeuroAffective Narrative Reconsolidation (NNR) process is described purely in cognitive-behavioural terms, it can be understood as a structured blend of imaginal exposure, hotspot processing, somatic monitoring, cognitive updating, and meaning reconstruction. The client activates the trauma memory in a controlled therapeutic context, identifies moments of peak emotional intensity, and gradually revisits these moments while introducing new information and interpretations that modify the original meaning of the event.
If the same process is described using EMDR terminology, it resembles targeted memory activation combined with a broader or more distributed attentional stance. The client maintains contact with the trauma memory while simultaneously remaining anchored in the present through breathing, bodily awareness, imagery, and environmental orientation. This widening of attention allows the nervous system to process the memory without becoming overwhelmed. The individual is not absorbed entirely by the traumatic scene; instead, part of awareness remains grounded in present safety. This dual attentional stance, characterised by maintaining a wider field of attention rather than a narrow focus, allows the memory to be revisited while reducing the likelihood that the nervous system will interpret the experience as a current threat.
What NA-CBT adds to these traditions is an explicit emphasis on the simultaneous engagement of physiology, affect, and cognition. Trauma recovery rarely occurs through cognitive insight alone. The body is not a secondary participant in the process; it is often the first system to detect danger and the last to recognise that the danger has passed. When therapy focuses solely on thought content, the body may continue to generate threat signals that override rational understanding.
From a neurobiological perspective, trauma is encoded not only as narrative memory but also as patterns of physiological activation. Tightness in the chest, tension in the abdomen, sudden shifts in breathing or heart rate, and waves of fear or nausea can all become embedded within the memory network. When these bodily responses are triggered, they can reactivate the emotional meaning of the trauma even when the individual intellectually understands that the event is over. In such circumstances, cognitive restructuring alone may feel like attempting to reason with an alarm system that continues to sound.
For this reason, regulation within NNR is not simply preparation for processing; it is an integral component of the processing itself. When breathing slows, bodily tension decreases, and the client learns to modulate distress while recalling the memory, new physiological information becomes encoded alongside the original memory trace. The nervous system gradually learns that the event belongs to the past rather than the present.
In this sense, physiological regulation becomes the bridge that enables cognitive updating to occur.
Affect Regulation Before Processing: Why TED Matters, and How It Helped Edward
For trauma processing to be possible, clients require more than psychological insight. They require physiological capacity. This capacity partly emerges from emotional regulation skills such as grounding techniques, progressive muscle relaxation, and body scanning. However, NA-CBT also places considerable emphasis on biological regulation through lifestyle stabilisation.
In clinical practice it becomes clear that trauma frequently disrupts fundamental biological rhythms. Sleep becomes fragmented or shallow, physical activity decreases or becomes associated with threat, and dietary patterns become irregular. These disruptions amplify emotional vulnerability. A fatigued nervous system reacts more strongly to stress, struggles to regulate fear responses, and finds it more difficult to tolerate the emotional activation required for trauma processing.
This is where the TED model becomes particularly relevant. In its original formulation, TED focuses on three biological systems that often become destabilised under chronic stress: tiredness (sleep regulation), exercise, and diet (hydration). Rather than treating these as peripheral wellbeing recommendations, NA-CBT frames them as integral components of emotional regulation (Mirea, 2025a, 2025b).
For Edward, the TED model became an important turning point in therapy because it helped him gradually rebuild trust in his body. Trauma had taught his nervous system that the body itself was dangerous. The injury had arrived suddenly and without warning, transforming what had once been a source of strength, his physical competence, into a site of vulnerability.
Processing trauma under such conditions can be difficult. Asking a client to revisit traumatic memories while their biological systems remain unstable is comparable to asking someone to rebuild a house while the foundations are still shifting beneath it.
We therefore began by stabilising sleep patterns. The aim was not perfection but rhythm. Edward began noticing that nights of better sleep were followed by days in which intrusive images were less vivid and his concentration improved. Even small improvements in sleep produced noticeable changes in emotional tolerance, reinforcing the importance of physiological regulation.
Exercise required particularly careful handling. For Edward, physical activity had become intertwined with threat because the injury occurred during boxing training. The gym was no longer a neutral space; it represented the moment his life changed. Rather than pushing him back toward high-intensity training, movement was reframed as a way of retraining the nervous system.
Initially this involved non-contact physical activity,exercise that communicated safety rather than competition or performance. Gentle training allowed his body to experience movement again without triggering the fear network associated with the trauma. Over time, the nervous system began to relearn a simple but powerful message: my body can move and nothing terrible happens. In this sense, exercise functioned both as behavioural activation and graded exposure within a NeuroAffective framework.
Dietary stabilisation also played an important role. Fluctuations in blood sugar, irregular eating patterns, and nutritional depletion can create physiological states that mimic anxiety or emotional instability. As Edward began eating more regularly and nourishing his body consistently, he noticed feeling less reactive and less physically unsettled. His emotional responses became more predictable and manageable.
By the time we entered Module 4 and began formal trauma processing, these physiological foundations proved essential. When Edward activated the trauma memory, he had internal resources available to regulate the experience. He could slow his breathing and genuinely experience its calming effects. He could observe bodily sensations without immediately interpreting them as signs of danger. The imagery of turning the distress dial downward became effective partly because his nervous system had already practised lowering arousal in everyday life.
From the perspective of NA-CBT, this illustrates a central principle: trauma processing is not something done to a memory in isolation. It is something done with a nervous system. The TED model helps prepare that nervous system so it can participate in the reconsolidation process rather than being overwhelmed by it.
Motivational Metaphors
In some contexts, TED may be reframed using alternative language that better reflects the client’s formulation, developmental stage, therapeutic goals, cultural background, or preferred way of making sense of their experiences. Such adaptations can enhance engagement, strengthen therapeutic alliance, and make key principles of self-regulation more accessible and personally meaningful.
These variations are primarily linguistic and motivational rather than theoretical. They do not alter TED’s core therapeutic role as an internalised “inner coach” that promotes self-regulation, physiological resilience, and adaptive self-care. The underlying principles of stabilising biological rhythms, strengthening personal agency, and enhancing the individual’s capacity for emotional regulation remain unchanged.
Examples include:
Tired – Exercise – Diet: the original physiological stabilisation framework, emphasising the regulation of sleep, physical activity, and nutrition as foundations for emotional wellbeing.
Train – Eat – Dream: supporting recovery following adversity or trauma by emphasising rebuilding strength, restoring hope, and fostering future orientation.
Time – Energy – Direction: facilitating recovery from stress and burnout through prioritisation, energy management, and values-guided action.
Trigger – Evaluate – Decide: promoting self-monitoring, impulse control, and more deliberate responding in emotionally charged situations.
Tension – Emotion – Defence: increasing awareness of bodily activation, affective states, and habitual protective responses that may maintain psychological distress.
These examples should be understood as motivational metaphors and mnemonic adaptations rather than distinct therapeutic protocols. They retain the spirit of TED as a practical and memorable framework for translating complex therapeutic principles into forms that clients can readily understand, personalise, and apply in everyday life.
TED and Behavioural Activation
Although TED shares certain features with Behavioural Activation (BA), the two approaches differ in their primary aims and underlying rationale. BA was originally developed within the treatment of depression and focuses predominantly on increasing engagement in meaningful, rewarding, and value-consistent activities in order to reduce avoidance and improve mood through environmental reinforcement. In contrast, TED emerged within NeuroAffective-CBT® as a broader self-regulation framework designed to strengthen the biological foundations that support emotional functioning.
Whereas BA primarily targets patterns of behavioural withdrawal and inactivity, often through activity monitoring and scheduling. TED focuses on stabilising physiological rhythms through interventions involving sleep, physical activity, nutrition, and other lifestyle domains relevant to the individual’s formulation. TED is therefore concerned not only with what individuals do, but also with the biological conditions under which psychological change becomes more achievable. From a NeuroAffective-CBT® perspective, disrupted sleep, poor nutrition, physical deconditioning, circadian instability, and chronic physiological dysregulation may significantly influence emotional vulnerability and the individual’s capacity to engage effectively in psychological treatment.
The two approaches are therefore complementary rather than competing. Behavioural Activation may increase behavioural engagement and access to reinforcement, while TED seeks to optimise the physiological and regulatory capacities that enable individuals to benefit more fully from therapeutic interventions, including behavioural change itself.
TED may therefore be conceptualised as creating the physiological conditions under which behavioural, cognitive, and emotional interventions can be more effectively utilised.
Closing Reflections
The Development of the Integrated-Self module is often the stage in therapy where a quiet but profound shift occurs. Many clients arrive feeling fragmented, as though their lives have been divided into two incompatible chapters: the person they were before the trauma and the person they became afterwards. Even when daily functioning resumes, the memory of the event can remain emotionally unfinished, intruding into the present through flashbacks and intense physiological reactions, accompanied by an unshakeable sense that danger still exists somewhere beneath the surface.
What clients often rediscover during this phase of therapy is not perfection or invulnerability, but continuity. They become able to look back at what happened without being pulled back into it. The event becomes part of their history rather than an ongoing threat. The nervous system no longer reacts as though the trauma is unfolding in the present moment.
In simple terms, the memory becomes exactly what it is meant to be: just one of the numerous memories once again, some are good memories, some are not so great…
The NeuroAffective Narrative Reconsolidation (NNR) protocol is one way of supporting that transition. It offers a structured framework that therapists can follow and refine while remaining flexible enough to meet each client’s nervous system where it currently is. Some individuals require more time in physiological stabilisation, while others move more quickly into narrative processing. What remains constant is the principle that trauma recovery requires cooperation between body, emotion, and cognition. Reliving the story alone is not sufficient, just as sensation alone is not sufficient. Healing often occurs when both are allowed to change together.
Within this process, trauma memories are not erased or suppressed; they are integrated. Clients learn that they can revisit the past while remaining anchored in the present. The memory gradually loses its power to dictate identity or future expectations. In many cases, it even becomes a source of meaning, strength, and personal insight, an experience that has been survived, understood, and woven into a broader narrative of the self.
One observation may resonate with many clinicians. It is not uncommon to meet clients who intellectually understand that their trauma is over yet continue to react to reminders with powerful bodily responses. They may say, “I know it’s over”, while still feeling their heart race, their stomach tighten, or their breath shorten when the memory arises.
From a neurobiological perspective, the explanation is straightforward: the body learns threat before the mind has time to interpret it.
And sometimes the body must learn safety before the mind can fully believe it. Integration is often the missing link. More often than not, it begins with helping the body learn what the mind already knows: it is over.
The therapeutic shifts described in NNR are consistent with emerging research on memory reconsolidation and emotional learning. When an emotionally significant memory is reactivated under conditions of relative safety and physiological regulation, the underlying memory trace may temporarily enter a labile state in which new contextual information can be incorporated before the memory is stored again (Nader and Hardt, 2009; Lane et al., 2015). During this reconsolidation window, previously threat-coded experiences can be updated through the integration of corrective emotional information, changes in autonomic regulation, and revised cognitive meaning.
From this perspective, the combination of narrative activation, physiological regulation, and cognitive updating used in NNR may facilitate conditions under which traumatic memories become re-encoded with reduced threat intensity and improved autobiographical integration. While further empirical research is required to directly test these mechanisms within the NA-CBT framework, current findings from affective neuroscience provide a plausible explanatory model for how integrated trauma processing may occur.
Clinical Implications and Future Research
The NeuroAffective Narrative Reconsolidation protocol illustrates how trauma processing can be approached through the coordinated engagement of physiological regulation, emotional processing, and cognitive updating. For clinicians, the model highlights the importance of preparing the nervous system for trauma work through stabilisation strategies, including affect regulation skills and biological rhythm restoration such as those described in the TED framework. The integration of somatic monitoring, narrative activation, and identity reconstruction offers a structured yet flexible approach that may help clients revisit traumatic memories while maintaining sufficient regulation to allow meaningful updating to occur. Importantly, the model emphasises that trauma processing is not solely a cognitive intervention but a whole-system process involving body, affect, and meaning.
Future research is required to examine the effectiveness of NA-CBT and the NNR protocol in controlled clinical settings. Empirical studies could explore treatment outcomes across different trauma populations and compare the model with established trauma therapies such as trauma-focused CBT and EMDR. Additional research may also investigate the neurobiological mechanisms underlying change, particularly the role of physiological regulation and memory reconsolidation processes in facilitating autobiographical integration. Such investigations would help clarify the therapeutic mechanisms involved and determine the potential contribution of NA-CBT within the broader landscape of evidence-based trauma interventions.
When such integration occurs, the trauma does not disappear from the person’s history, but it loses its power to dominate the present, becoming part of a life story that can be remembered, understood, and carried forward without fear.
Brown, B. (2012) Daring Greatly. New York: Gotham Books.
Ehlers, A. and Clark, D.M. (2000) ‘A cognitive model of post-traumatic stress disorder’, Behaviour Research and Therapy, 38(4), pp. 319–345.
Hackmann, A., Bennett-Levy, J. and Holmes, E.A. (eds.) (2011) The Oxford guide to imagery in cognitive therapy. Oxford: Oxford University Press.
Lane, R.D., Ryan, L., Nadel, L. and Greenberg, L. (2015) ‘Memory reconsolidation, emotional arousal, and the process of change in psychotherapy: new insights from brain science’, Behavioral and Brain Sciences, 38, e1.
LeDoux, J. (2015) Anxious: Using the Brain to Understand and Treat Fear and Anxiety. New York: Viking.
Nader, K. and Hardt, O. (2009) ‘A single standard for memory: the case for reconsolidation’, Nature Reviews Neuroscience, 10(3), pp. 224–234.
Shapiro, F. (2018) Eye Movement Desensitization and Reprocessing (EMDR) Therapy. 3rd edn. New York: Guilford Press.
Clinical Note The case illustration presented in this article is anonymised and partially modified for confidentiality. NeuroAffective Narrative Reconsolidation (NNR) is intended for use by trained mental health professionals within appropriate clinical settings.