

Pain is not simply a signal travelling from the body to the brain. It is a neuroaffective experience emerging from the continuous interaction between physiology, emotion, cognition, and context.
Daniel Mirea (June, 2026)
NeuroAffective-CBT® | https://neuroaffectivecbt.com

Abstract
Pain has traditionally been conceptualised as a direct consequence of tissue damage, whereby nociceptive signals travel from the body to the brain and are subsequently perceived as pain. However, contemporary neuroscience suggests that this explanation is incomplete. Modern pain science increasingly recognises pain as a multidimensional neurobiological and psychological experience that emerges from the continuous interaction between sensory information, emotional states, memory, learning, expectation, context, and prediction. This article explores the distinction between nociception and pain, reviews the role of spinal gating and descending modulation pathways, and examines how affective and cognitive processes contribute to the conscious experience of pain. Drawing upon developments in affective neuroscience, cognitive neuroscience, and contemporary pain research, the article proposes that pain is best understood as a neuroaffective phenomenon rather than a simple sensory event. A NeuroAffective-CBT® (NA-CBT®) perspective is presented, conceptualising pain as the product of an ongoing interaction between the body, brain, and affective systems. Understanding pain through this integrative framework may help clinicians and individuals alike appreciate why pain can persist in the absence of ongoing tissue damage and why effective treatment often requires a biopsychosocial and neuroaffective approach.
Keywords: Pain, Nociception, NeuroAffective-CBT®, Chronic Pain, Affective Neuroscience, Central Sensitisation, Predictive Processing, Pain Perception, Cognitive Behavioural Therapy, Neuroaffective Formulation
The Traditional View of Pain
Although pain has been extensively studied within medicine, neuroscience, and rehabilitation disciplines, discussions within psychotherapy have often focused primarily on symptom management rather than on understanding pain as a complex neuroaffective experience. From a NeuroAffective-CBT perspective, this distinction is important because many of the emotional difficulties presented in therapy involve physiological distress that is experienced, interpreted, and responded to in ways that closely resemble the mechanisms observed in pain itself.
Therefore, pain is not simply something we detect. It is something we experience. And experiences emerge from the continuous conversation between the body, the brain, and affect.
Most of us have been taught a relatively simple explanation of pain. You step on a nail. The injured tissue sends a pain signal through the nerves. The signal travels up the spinal cord.
The brain receives the message. You feel pain.
Simple. Logical. Intuitive.
And yet, although this explanation contains some truth, it is only part of the story.
Over the last several decades, advances in neuroscience, psychology, pain medicine, and affective neuroscience have fundamentally changed our understanding of pain. What we once believed to be a straightforward sensory process is now understood to be a far more complex interaction between the body, brain, emotions, memories, beliefs, expectations, and context.
In many ways, pain provides one of the clearest examples of how the body, brain, and affective systems continuously interact to shape our lived experience.
Most educational diagrams describe pain as a four-step process:
1. Detection of Potential Harm
Specialised nerve endings known as nociceptors detect potentially harmful stimuli such as:
- Extreme heat
- Excessive pressure
- Tissue injury
- Chemical irritation
These receptors are often described as “pain receptors,” although this is not entirely accurate.
Their actual role is to detect potential danger.
When activated, they send electrical signals through peripheral nerves toward the spinal cord.
2. The Spinal Gate
The signal reaches the spinal cord, where information is filtered before continuing toward the brain.
This concept originates from the famous Gate Control Theory of Pain, proposed by Ronald Melzack and Patrick Wall in 1965.

According to this theory, the spinal cord functions somewhat like a gatekeeper.
Some signals are allowed through. Others are dampened. Others may be amplified.
This explains why rubbing an injured area often reduces discomfort. Touch signals can partially compete with and inhibit nociceptive input at spinal cord level.
3. Modulation
Signals reaching higher centres of the nervous system can be increased or decreased by descending pathways from the brainstem.
In some situations, pain can be dramatically suppressed.
Examples include:
- Soldiers injured in battle
- Athletes finishing a race despite serious injuries
- Emergency situations where survival is prioritised
Conversely, pain can also be amplified by stress, anxiety, fear, sleep deprivation, inflammation, or sensitisation.
4. Conscious Perception
If sufficient information reaches the brain, pain becomes consciously experienced.
This is where most simplified diagrams end.
However, this is also where the most interesting part of the story begins.
The Biggest Misunderstanding About Pain
Perhaps the most important discovery in modern pain science is this:
Pain signals are not actually pain.
The nerves do not carry pain itself.
They carry information.
They carry evidence.
They carry warning signals.
What travels through the nervous system is better described as:
Nociception
Nociception refers to the detection and transmission of potentially harmful stimuli.
Pain, however, is something different.
Pain is an experience.
And experiences are generated by the brain.
This distinction may sound subtle, but it changes everything.
Nociception Without Pain
Consider the following examples.
A footballer breaks a bone during an important match and continues playing.
A soldier is shot in combat and reports little or no pain until reaching safety.
An individual involved in a car accident walks around helping others before realising they are injured.
In all these situations:
The injury exists.
The nociceptive signals exist.
Yet the pain experience is significantly reduced or absent. The nervous system has decided that survival is currently more important than suffering.
Pain Without Injury
Now consider the opposite situation.
An individual experiences severe chronic pain despite normal scans and medical investigations.
Someone develops phantom limb pain after amputation.
A person with fibromyalgia experiences widespread pain despite no obvious tissue damage.
An individual suffers debilitating migraines despite no visible injury.
In these situations, pain exists. Yet tissue damage may be minimal or absent. Again, pain cannot simply be explained as a direct readout of injury.
Something else is happening.
The Brain Is Not Reading Pain
A common misconception is that the brain acts like a computer reading incoming messages. The reality is far more sophisticated.
Modern neuroscience increasingly supports the idea that the brain functions as a prediction machine. Rather than passively waiting for information, the brain continuously asks:
“What is happening?”
“How dangerous is it?”
“What should I do about it?”
Pain appears to emerge from the brain’s attempt to answer these questions.
The human brain rapidly combines incoming sensory information with previous experiences, memory, learning, expectations, emotional state, beliefs, current stress levels, and environmental context before constructing the experience we call pain.
Pain is therefore not merely detected. Pain is actively constructed by the brain based upon incoming information, prior learning, emotional state, and context.
Why Context Matters
Imagine stepping on the same object under different circumstances.
Scenario One:
You are walking barefoot through your garden.
You step on a sharp object unexpectedly.
Pain is immediate.
Scenario Two:
You are undergoing a medical procedure.
You know discomfort is expected.
You trust the clinician.
The same level of stimulation may feel significantly less painful.
Scenario Three:
You are highly anxious, exhausted, sleep deprived, and worried about your health.
The exact same physical stimulus may feel dramatically worse.
The tissue has not changed.
The brain’s interpretation has changed.
The Emotional Brain and Pain
One of the greatest limitations of many pain models is that they largely ignore emotion. Pain is not simply sensory. Pain is profoundly emotional. Several brain regions contribute to the experience.
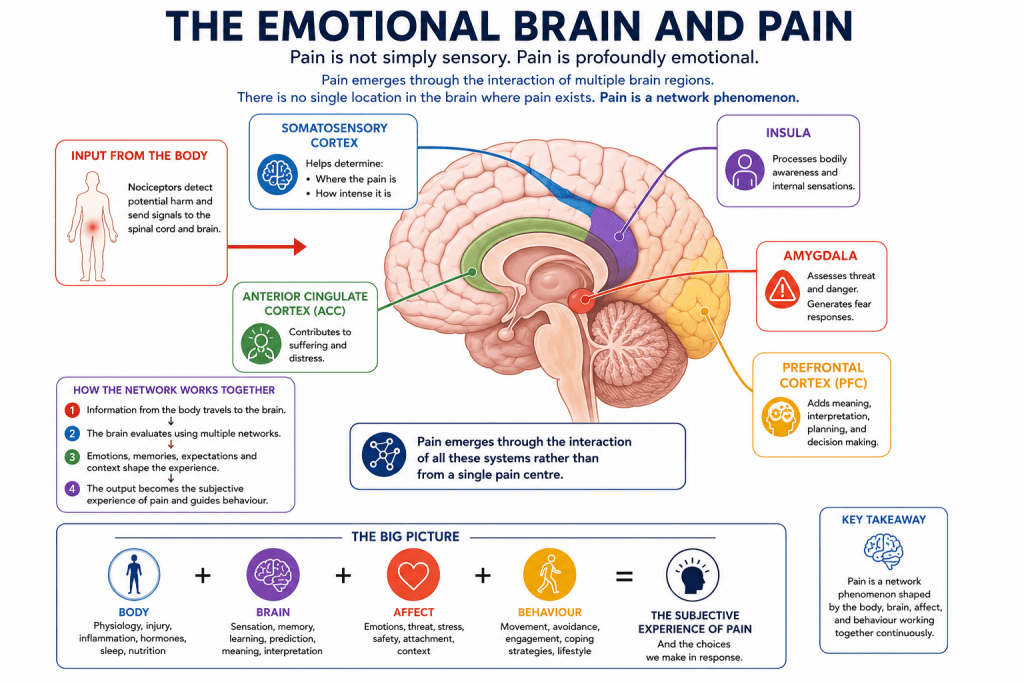
Somatosensory Cortex
Helps determine (1) Where the pain is (2) How intense it is
Insula
Processes bodily awareness and internal sensations.
Anterior Cingulate Cortex
Contributes to suffering and distress.
Amygdala
Assesses threat and danger.
Generates fear responses.
Prefrontal Cortex
Adds meaning, interpretation, planning, and decision making.
Pain emerges through the interaction of all these systems rather than from a single pain centre.
There is no single location in the brain where pain exists.
Pain is a network phenomenon.
Fear Can Increase Pain
Imagine touching a hot stove.
The immediate pain serves an adaptive purpose.
You withdraw your hand.
Problem solved.
However, if the nervous system begins associating many harmless experiences with danger, pain can become amplified.
The more fearful we become of pain:
- The more we monitor it
- The more we anticipate it
- The more attention we give it
The more significant it can become.
This does not mean the pain is imaginary.
It means the nervous system is becoming increasingly protective.
In many chronic pain conditions, the alarm system becomes overly sensitive.
The danger detector becomes too good at its job.
What Chronic Pain Teaches Us
Acute pain protects us.
Chronic pain often reflects protection that has become excessive.
The nervous system learns.
The brain learns.
The body learns.
Neural pathways become strengthened through repetition.
Eventually the system may begin generating pain responses disproportionate to actual tissue damage.
This process is often referred to as:
- Central sensitisation
- Neural amplification
- Pain sensitisation
The pain remains real.
The suffering remains real.
The underlying mechanisms, however, are different from those involved in acute injury.
A NeuroAffective-CBT Perspective
Within NeuroAffective-CBT, pain can be understood through the interaction between three continuously communicating systems:
Body
The body provides physiological information.
This includes:
- Injury
- Inflammation
- Hormonal changes
- Sleep quality
- Nutrition
- Energy availability
- Physical conditioning
Brain
The brain interprets incoming information.
It generates predictions based upon:
- Previous experiences
- Memory
- Learning
- Core beliefs
- Expectations
Affect
Affective systems shape emotional meaning.
These include:
- Fear
- Shame
- Anxiety
- Helplessness
- Anger
- Grief
Together these systems create the subjective experience we call pain.
Within NeuroAffective-CBT, emotional pain and physical pain are not viewed as entirely separate phenomena. Both involve physiological activation, affective meaning-making, cognitive interpretation, and behavioural responses. Clients frequently describe emotional suffering using physical language: a heavy chest, a knot in the stomach, emotional exhaustion, pressure, tension, emptiness, or feeling broken. Understanding pain therefore provides an important framework for understanding emotional suffering itself.
The Core Principle of NeuroAffective-CBT
The Body influences the Brain.
The Brain influences Affect.
Affect influences Behaviour.
Behaviour influences Physiology.
When any part of this system becomes dysregulated, suffering may emerge.
When all parts of the system are addressed together, healing becomes possible.
Why This Matters Clinically
Understanding pain differently changes how we approach treatment.
Rather than asking only:
“Where is the damage?”
We might also ask:
- What is the nervous system trying to protect?
- What role is stress playing?
- What role is sleep playing?
- What role is fear playing?
- What role is emotional suppression playing?
- What role is avoidance playing?
- What role is physical deconditioning playing?
- What role is chronic activation of threat systems playing?
These questions do not invalidate physical explanations.
They expand them.
Pain Is Real, Even When Scans Are Normal
One of the most harmful misconceptions encountered in clinical practice is the belief that normal scans mean symptoms are “all in the mind.”
Nothing could be further from the truth.
Modern neuroscience demonstrates that:
- Pain is real.
- The nervous system is real.
- Brain-based processing is real.
- Emotional amplification is real.
- Sensitisation is real.
The absence of visible tissue damage does not invalidate suffering.
It simply means the explanation may be more complex than originally assumed.
The Future of Pain Science
Pain science continues to evolve.
Increasingly, researchers are recognising the importance of integrating:
- Neuroscience
- Psychology
- Physiology
- Immunology
- Lifestyle medicine
- Sleep science
- Exercise science
- Nutritional psychiatry
- Metabolic psychiatry
into a more comprehensive understanding of human suffering.
Pain cannot be fully understood through tissue damage alone.
Nor can it be fully understood through psychology alone.
The future almost certainly lies in integration.
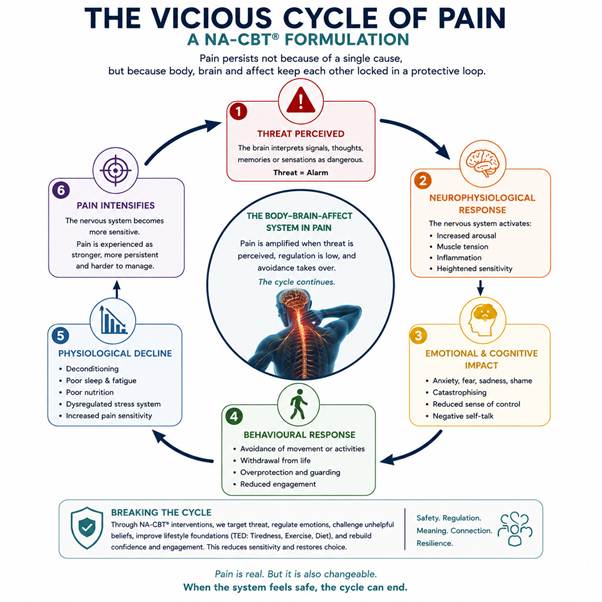
A NeuroAffective-CBT Formulation of Pain
From a NeuroAffective-CBT perspective, pain cannot be fully understood through a purely biomedical model, nor can it be adequately explained through a purely psychological framework. Rather, pain emerges from the dynamic interaction between physiological processes, affective systems, and cognitive interpretation. This perspective is consistent with the NA-CBT Body–Brain–Affect Triangle, which proposes that emotional and behavioural experiences arise from the continuous bidirectional communication between bodily states, brain-based processing, and affective meaning-making systems.
Within this framework, the body provides ongoing physiological information regarding injury, inflammation, fatigue, energy availability, sleep quality, nutrition, hormonal changes, and physical conditioning. The brain continuously interprets this information through the lens of prior learning, autobiographical memory, expectations, beliefs, and threat predictions. Simultaneously, affective systems assign emotional meaning to incoming experiences, influencing whether bodily sensations are perceived as manageable, threatening, overwhelming, or catastrophic.
Consequently, pain is not viewed as a simple readout of tissue damage but rather as a neuroaffective experience generated by the interaction of these multiple systems.
The Role of Threat Perception
One of the central assumptions within NA-CBT is that the nervous system is fundamentally organised around safety and survival. The brain continuously evaluates internal and external information to determine the level of threat present in any given situation.
When a stimulus is interpreted as dangerous, the nervous system may increase vigilance, muscular tension, autonomic arousal, and pain sensitivity. Conversely, when safety cues are present, physiological regulation improves, threat responses diminish, and pain intensity may decrease.
Importantly, threat perception is not determined solely by objective reality. It is influenced by previous experiences, trauma histories, attachment experiences, health beliefs, social context, and emotional states.
Two individuals may therefore experience the same physical injury in dramatically different ways depending upon how their nervous systems interpret and respond to the event.
Trauma, Emotional Learning, and Pain Amplification
Traumatic experiences can significantly alter the way the nervous system responds to future threats. Individuals who have experienced chronic adversity, abuse, neglect, medical trauma, bullying, or emotionally invalidating environments may develop heightened sensitivity within threat-detection systems.
Over time, the nervous system may become increasingly efficient at detecting danger, sometimes responding to relatively minor stimuli as though they represent significant threats.
Within the NA-CBT model, unresolved trauma memories may continue to influence present-day physiological and emotional reactions long after the original event has passed. Pain can therefore become linked not only to tissue-based signals but also to fear networks, emotional memories, learned associations, and protective behavioural patterns.
This perspective aligns with contemporary research demonstrating the involvement of the amygdala, anterior cingulate cortex, insula, hippocampus, and prefrontal regions in both pain processing and emotional regulation.
The Influence of Shame and Anxiety
NA-CBT places particular emphasis on the role of shame-based emotional schemas and chronic anxiety in maintaining emotional distress and self-sabotaging patterns.
Shame frequently operates as a hidden amplifier of suffering.
Individuals who carry longstanding beliefs such as:
- “I am weak.”
- “I should be coping better.”
- “There must be something seriously wrong with me.”
- “Nobody understands what I am going through.”
may experience increased emotional distress alongside physical symptoms.
Similarly, chronic anxiety can maintain heightened physiological arousal, increased muscle tension, sleep disruption, hypervigilance, and persistent monitoring of bodily sensations. These processes may inadvertently reinforce pain pathways and increase the perceived intensity of symptoms.
From a neuroaffective perspective, emotional suffering and physical suffering often become intertwined, creating self-reinforcing cycles that can be difficult to break without targeted intervention.
The Original TED Model: Tired, Exercise, and Diet
A central component of the NeuroAffective-CBT framework is the original TED model, which focuses on three fundamental physiological domains that frequently influence emotional wellbeing, stress tolerance, cognitive functioning, and pain perception:
Tiredness, Exercise, and Diet.
Within NA-CBT, TED is often conceptualised as an individual’s internal physiological coach. Before attempting to understand complex emotional reactions, trauma responses, self-sabotaging behaviours, or chronic distress, clinicians are encouraged to assess the extent to which these three biological domains may be influencing the individual’s current functioning.
Tiredness
Sleep deprivation and chronic fatigue can significantly alter the way the nervous system processes both emotional and physical experiences.
Research consistently demonstrates that insufficient sleep is associated with:
- Increased pain sensitivity
- Reduced emotional regulation
- Heightened threat perception
- Increased anxiety and irritability
- Poorer stress tolerance
- Reduced cognitive flexibility
- Greater physiological arousal
From a neuroaffective perspective, an exhausted nervous system is often a more reactive nervous system.
Individuals experiencing chronic pain frequently report poor sleep quality, whilst poor sleep itself can increase pain intensity, creating a self-perpetuating cycle of distress and physiological dysregulation.
For this reason, improving sleep and recovery is often considered a foundational intervention within the NA-CBT model before attempting more intensive emotional processing work.
Exercise
Physical activity plays a critical role in both emotional and physiological regulation.
Regular movement influences multiple systems associated with pain modulation, including:
- Endorphin release
- Stress regulation
- Neuroplasticity
- Cardiovascular health
- Inflammatory processes
- Mood regulation
- Self-efficacy and resilience
Importantly, exercise may also help challenge fear-avoidance patterns commonly observed in chronic pain conditions.
Many individuals gradually reduce activity levels because movement becomes associated with discomfort or fear of injury. Whilst avoidance may provide short-term relief, prolonged inactivity can contribute to deconditioning, increased vulnerability, reduced confidence, and further sensitisation of the nervous system.
Within NA-CBT, exercise is therefore viewed not simply as a physical intervention but also as a psychological and neurobiological regulator capable of influencing both mood and pain perception.
Diet
Nutrition provides the biological foundation upon which the brain and body operate.
Emerging evidence from nutritional psychiatry, metabolic psychiatry, and neuroscience increasingly suggests that dietary factors may influence emotional wellbeing, inflammation, energy production, cognitive functioning, and stress resilience.
Poor nutritional habits may contribute to:
- Fatigue
- Metabolic dysfunction
- Increased inflammation
- Blood sugar instability
- Reduced concentration
- Mood fluctuations
- Poor recovery capacity
From an NA-CBT perspective, diet is not viewed through a restrictive or purely weight-focused lens. Rather, it is considered a crucial component of physiological regulation that may influence how effectively the nervous system responds to both emotional and physical stressors.
TED and Pain Perception
The relevance of the TED model to pain becomes increasingly apparent when viewed through a neuroaffective lens.
An individual who is:
- Chronically sleep deprived,
- Physically deconditioned,
- Nutritionally dysregulated,
may experience a nervous system that is more reactive, more vigilant, and more sensitive to both internal and external stressors.
Consequently, pain intensity may increase even when tissue damage remains unchanged.
Conversely, improvements in sleep, physical conditioning, and nutritional stability may help reduce physiological stress, improve emotional regulation, increase resilience, and support healthier pain modulation pathways.
Within the NeuroAffective-CBT framework, TED therefore represents far more than a lifestyle intervention.
It represents a foundational physiological platform upon which emotional regulation, cognitive flexibility, behavioural change, trauma processing, and recovery can occur.
When individuals begin addressing tiredness, exercise, and diet simultaneously, they are often not simply improving their physical health. They are creating the biological conditions necessary for the nervous system to feel safer, more regulated, and less protective.
From this perspective, the TED model becomes directly relevant to understanding why some individuals remain trapped within cycles of chronic pain, emotional distress, and physiological dysregulation, whilst others gradually move towards recovery and resilience.
Metabolic Health, Ketogenic Therapies and Pain
Over recent years, growing attention has been directed towards the relationship between metabolic health, inflammation, brain function, emotional wellbeing, and chronic illness. Whilst traditionally associated with weight management or epilepsy treatment, ketogenic therapies are increasingly being investigated for their potential effects on neurological, psychiatric, and inflammatory conditions.
As discussed in a recent NeuroAffective-CBT article exploring ketogenic therapies and mental health, emerging research suggests that metabolic dysfunction may influence psychological wellbeing through mechanisms involving inflammation, mitochondrial function, oxidative stress, insulin resistance, and energy metabolism within the brain.
This perspective aligns closely with one of the central assumptions of the NA-CBT model: the brain does not function independently from the body. Physiological dysregulation may influence emotional wellbeing, whilst emotional distress may simultaneously influence physiological functioning.
The relevance of this emerging field to pain should not be underestimated.
Many chronic pain conditions are now recognised to involve not only structural or tissue-based factors but also inflammatory processes, autonomic dysregulation, altered stress responses, sleep disturbance, and changes in central nervous system functioning. Increasingly, researchers are exploring whether metabolic interventions may influence some of these mechanisms.
As stated in the recent NeuroAffective-CBT review of ketogenic therapies:
“The question is not whether ketogenic therapies represent a miracle cure. The question is whether some of the benefits reported by patients may be explained by improvements in physiological regulation, inflammation, energy metabolism, sleep, cognition, and emotional stability.”
This is an important distinction.
Within NA-CBT, ketogenic diets are not conceptualised as psychological treatments. Rather, they may represent one example of how physiological interventions can potentially influence the Body–Brain–Affect system.
For some individuals, improvements in metabolic health may be associated with:
- Reduced systemic inflammation
- Improved energy regulation
- Enhanced cognitive clarity
- Better sleep quality
- Reduced emotional volatility
- Improved stress tolerance
All of which may indirectly influence the experience of pain.
Further research is required before definitive conclusions can be reached. However, the growing field of metabolic psychiatry reinforces a principle that sits at the heart of NeuroAffective-CBT®:
The body influences the brain. The brain influences affect. Affect influences behaviour. Behaviour influences physiology.
Understanding pain therefore requires us to look beyond symptoms alone and consider the broader physiological and emotional ecosystem within which those symptoms occur.
Towards an Integrated Understanding of Pain
The clinical implications of this model are significant.
Rather than asking solely:
“Where is the injury?“
NA-CBT® encourages clinicians and individuals to also ask:
- What is the nervous system trying to protect?
- What emotional meanings have become attached to the symptoms?
- What role is fear playing?
- What role is shame playing?
- What role is avoidance playing?
- What role is trauma playing?
- What role are sleep, nutrition, and physical conditioning playing?
- What factors are maintaining the brain’s prediction that danger remains present?
These questions do not deny the reality of pain.
Instead, they acknowledge the complexity of human suffering and provide a broader framework for understanding why pain may persist long after tissue healing has occurred.
Ultimately, the NeuroAffective-CBT® model views pain as a whole-person experience emerging from the continuous interaction between the body, brain, and affective systems. By addressing all three domains simultaneously, clinicians may be better positioned to help individuals reduce suffering, improve functioning, and develop a more integrated relationship with their physical and emotional experiences.
Final Thoughts
Perhaps the most important lesson from modern pain science is this:
Pain is not simply a signal travelling from the body to the brain.
Pain is a dynamic neurobiological experience emerging from the continuous interaction between bodily information, emotional states, prior learning, memory, beliefs, context, and prediction.
The body provides information.
The brain evaluates that information.
The affective system gives it meaning.
Together they create the conscious experience we call pain.
Understanding this complexity does not make pain less real.
If anything, it helps explain why pain can sometimes persist long after tissue healing has occurred, why emotions can influence symptoms, why stress can worsen discomfort, and why genuinely effective treatment often requires us to address the whole person rather than a single body part.
In many respects, pain may be one of the clearest demonstrations that human beings cannot be reduced to either mind or body alone.
We are, and always have been, an integrated neuroaffective system.
References
Apkarian, A.V., Baliki, M.N. and Geha, P.Y. (2009) ‘Towards a theory of chronic pain’, Progress in Neurobiology, 87(2), pp. 81–97.
Atlas, L.Y. and Wager, T.D. (2012) ‘How expectations shape pain’, Neuroscience Letters, 520(2), pp. 140–148.
Craig, A.D. (2003) ‘A new view of pain as a homeostatic emotion’, Trends in Neurosciences, 26(6), pp. 303–307.
Eccleston, C. and Crombez, G. (1999) ‘Pain demands attention: A cognitive-affective model of the interruptive function of pain’, Psychological Bulletin, 125(3), pp. 356–366.
Fields, H.L. (2004) ‘State-dependent opioid control of pain’, Nature Reviews Neuroscience, 5(7), pp. 565–575.
Flor, H. (2003) ‘Cortical reorganisation and chronic pain: Implications for rehabilitation’, Journal of Rehabilitation Medicine, 35(S41), pp. 66–72.
Gatchel, R.J., Peng, Y.B., Peters, M.L., Fuchs, P.N. and Turk, D.C. (2007) ‘The biopsychosocial approach to chronic pain: Scientific advances and future directions’, Psychological Bulletin, 133(4), pp. 581–624.
LeDoux, J.E. (2015) Anxious: Using the Brain to Understand and Treat Fear and Anxiety. New York: Viking.
Melzack, R. (1999) ‘From the gate to the neuromatrix’, European Journal of Pain, 3(Suppl A), pp. 121–126.
Melzack, R. and Wall, P.D. (1965) ‘Pain mechanisms: A new theory’, Science, 150(3699), pp. 971–979.
Mirea, D. (2018) Describing NeuroAffective-CBT®: An integrative model of psychological distress and emotional regulation. NeuroAffective-CBT®. Available at: https://neuroaffectivecbt.com (Accessed: 1 June 2026).
Mirea, D. (2025) TED in NeuroAffective-CBT®: An applied self-regulation framework for enhancing emotional wellbeing through sleep, movement and nutrition. NeuroAffective-CBT®, 10 December. Available at: https://neuroaffectivecbt.com/2025/12/10/ted-in-neuroaffective-cbt-an-applied-self-regulation-framework-for-enhancing-emotional-well-being-through-sleep-movement-and-nutrition/ (Accessed: 1 June 2026).
Mirea, D. (2026) Could altering brain metabolism improve emotional wellbeing? Exploring ketogenic therapies through a NeuroAffective-CBT® lens. NeuroAffective-CBT®. Available at: https://neuroaffectivecbt.com (Accessed: 1 June 2026).
Moseley, G.L. and Butler, D.S. (2017) Explain Pain Supercharged. Adelaide: Noigroup Publications.
Nader, K. and Hardt, O. (2009) ‘A single standard for memory: The case for reconsolidation’, Nature Reviews Neuroscience, 10(3), pp. 224–234.
Panksepp, J. (1998) Affective Neuroscience: The Foundations of Human and Animal Emotions. Oxford: Oxford University Press.
Schubiner, H. and Betzold, M. (2021) Unlearn Your Pain. Boulder, CO: Mind Body Publishing.
Tracey, I. and Mantyh, P.W. (2007) ‘The cerebral signature for pain perception and its modulation’, Neuron, 55(3), pp. 377–391.
Turk, D.C. and Gatchel, R.J. (2018) Psychological Approaches to Pain Management: A Practitioner’s Handbook. 3rd edn. New York: Guilford Press.
Vlaeyen, J.W.S. and Linton, S.J. (2000) ‘Fear-avoidance and its consequences in chronic musculoskeletal pain’, Pain, 85(3), pp. 317–332.
Wiech, K. (2016) ‘Deconstructing the sensation of pain: The influence of cognitive processes on pain perception’, Science, 354(6312), pp. 584–587.
