

Defining Perimenopause and Menopause
Perimenopause is often approached primarily as a hormonal issue and is typically managed within general medical practice. While this is appropriate, it may underrepresent the broader impact of this transition across neural, behavioural, and regulatory systems. As a result, the condition is not consistently addressed within the field of psychotherapy. From a NeuroAffective-CBT perspective, perimenopause can be understood as a multi-system recalibration involving the brain, body, and behaviour, with direct implications for clinical formulation and support.
Perimenopause refers to the transitional period leading up to menopause, during which ovarian hormone production becomes increasingly variable. This phase may begin several years before the final menstrual period and is characterised by fluctuations in estrogen and progesterone levels, often accompanied by changes in menstrual regularity, sleep, mood, and physiological stability.
Menopause is clinically defined as the point at which menstruation has ceased for twelve consecutive months, marking the end of reproductive function (National Institute for Health and Care Excellence, 2024). Postmenopause refers to the phase following this transition, during which hormone levels stabilise at a lower baseline.
From a physiological perspective, perimenopause represents a continuous process of endocrine adjustment rather than a discrete event. It is characterised by fluctuating hormone levels and associated changes in sleep, mood, and cognitive function (National Institute for Health and Care Excellence, 2024). From a NeuroAffective-CBT perspective, this transition can be understood as a biopsychophysiological process in which these changes increase regulatory load across multiple interacting systems.
The transition from the reproductive years into this phase involves a significant endocrine shift, characterised primarily by declining estrogen and progesterone levels (Mirea and Popa, 2026). These hormonal changes do not affect a single system in isolation. Estrogen receptors are widely distributed across the brain, cardiovascular tissue, skeletal muscle, bone, and immune structures, meaning that changes in estrogen signalling influence multiple interconnected physiological systems simultaneously (Strasser, 2015; Mennitti et al., 2024).
Brain and Neurochemical Regulation
The central nervous system is directly involved in this transition. Estrogen crosses the blood–brain barrier and modulates neural function through its effects on receptor expression, synaptic plasticity, and neurotransmitter dynamics. In particular, estrogen interacts with serotonergic pathways, influencing serotonin synthesis, receptor sensitivity, and reuptake processes.
Fluctuations or sustained reductions in estrogen during perimenopause and menopause have been associated with changes in mood stability, increased vulnerability to anxiety, reduced cognitive clarity, and the commonly reported experience of “brain fog.” These outcomes are multifactorial; however, altered stress responsivity and changes in neuroplastic processes are recognised contributors to emotional and cognitive shifts (Davidson and McEwen, 2012; Deslandes, 2014).
Gut–Brain–Immune Interactions
Serotonin regulation is not confined to the brain. Approximately 90% of serotonin is synthesised in the gastrointestinal tract. Although peripheral serotonin does not directly cross the blood–brain barrier, the gut microbiome influences central nervous system function through immune signalling, vagal pathways, and metabolite production, a bidirectional system often described as the gut–brain axis.
Emerging evidence suggests further interaction between estrogen metabolism and the gut microbiome via the estrobolome, the collection of microbial genes capable of metabolising estrogens (Plottel and Blaser, 2011). After hepatic processing, conjugated estrogens enter the intestinal tract, where microbial enzymes may influence their reactivation and recirculation.
In parallel, short-chain fatty acids (SCFAs), produced by specific bacterial populations, contribute to gut barrier integrity, immune modulation, and metabolic regulation. During perimenopause, shifts in estrogen levels may coincide with changes in microbiome composition, with potential downstream effects on inflammatory tone and stress-related physiology (Gleeson et al., 2011; Nieman, 2018).
A System in Ongoing Dialogue
Taken together, endocrine, neural, immune, and microbial systems operate in continuous interaction. When estrogen signalling declines, the balance of regulatory processes across these systems may shift, influencing metabolic health, mood stability, energy regulation, and cognitive clarity.
From this perspective, the experience of perimenopause is not reducible to a single mechanism. Rather, it reflects the convergence of multiple regulatory changes occurring simultaneously across the organism.
NA-CBT Implications: Supporting Regulation During Transition
The day-to-day manifestations of this recalibration are both physiological and psychological. Changes in sleep quality, stress tolerance, digestion, appetite, mood stability, and cognitive function may reflect underlying shifts in hormonal, neural, and gut–brain signalling; presenting complaints are common across a range of psychiatric conditions therefore diagnosis and mental health assessment is difficult.
Within the NA-CBT framework, these changes are understood not simply as symptoms to be eliminated, but as indicators of altered regulatory load within the system.
This perspective reinforces the importance of stabilising core regulatory domains:
- Sleep: maintaining consistent timing and protecting recovery
- Exercise: particularly resistance training, to support neuromuscular and metabolic stability
- Nutrition: ensuring adequate protein, fibre, alcohol reduction and energy availability
- Stress regulation: supporting transitions between activation and recovery
These are not quick fixes. They function as foundational supports for a system undergoing biological recalibration.
The Body–Brain–Affect Relationship
As outlined above, the body–brain–affect connection is central to how the organism functions as an integrated system. Early work by Charles Darwin (1872) recognised that affective expression is a core feature of emotional states and contributes to subjective experience. More recent research, including work by David J. Anderson (2014 and 2016), has further explored the neural circuits underlying behavioural responses, demonstrating how hormones and neuromodulators shape contextual affective states through signals experienced as feelings, imagery, and automatic behavioural tendencies.
From this perspective, the perimenopausal transition can be understood as a complex interaction of hormonal change, affective fluctuation, and behavioural shifts. Translating these processes into psychotherapy highlights the importance of understanding how to support exposure, regulation, and recovery in a safe and compassionate manner, with the aim of improving quality of life.
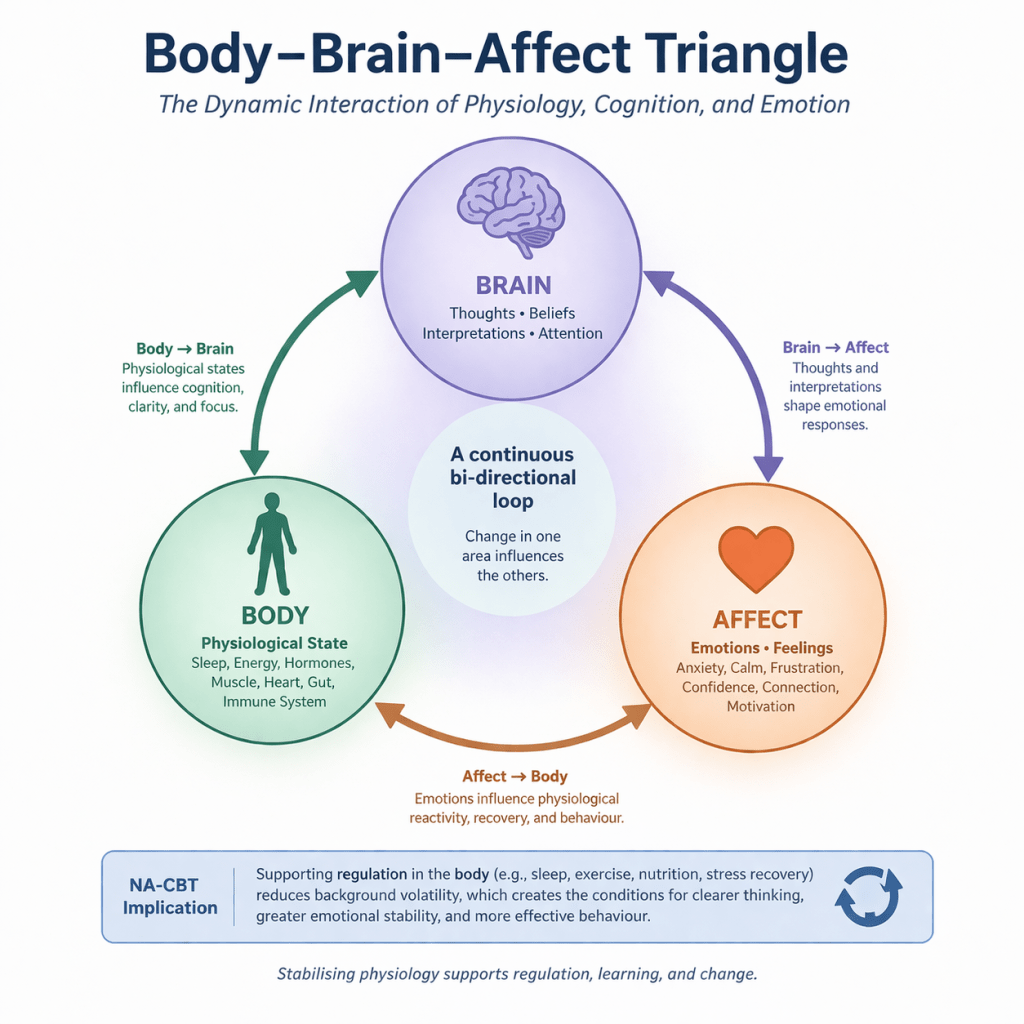
As illustrated in the Body–Brain–Affect model, this relationship provides a clinically useful framework for formulation:
- Physiological states shape emotional and cognitive processes
- Emotions influence thoughts and behaviour
- Thoughts and behaviours, in turn, reshape physiology
Within this system, the TED model (Tired – Exercise – Diet) functions as the physiological regulation arm of NA-CBT, reducing background volatility so that deeper psychological learning can occur.
A central therapeutic aim is supporting clients in distinguishing between:
- Raw affect — the body’s immediate signal of threat or discomfort
- Interpretation — the meaning the mind assigns to that signal
When these become fused, emotions may be experienced as overwhelming, self-defining, or difficult to regulate. Stabilising physiological state first helps create the conditions for more flexible interpretation and response.
Why Lifestyle Interventions Belong Inside Psychotherapy
When sleep is disrupted, movement is limited, or metabolic stability is compromised, individuals often experience:
- heightened anxiety or irritability
- increased emotional reactivity and rumination
- intensified self-criticism or shame
- reduced tolerance for uncertainty, stress, or interpersonal challenge
From an NA-CBT perspective, these are not failures of insight or willpower. They reflect a system operating under strain and psychotherapeutic intervention without emotional recalibration is difficult. The TED model aims for sufficiency rather than optimisation. The goal is not perfect habits, but a stable internal environment that reduces threat sensitivity and supports emotional regulation.
Illustrative Case Example
A 47-year-old woman presented with anxiety and work-related stress, without initial awareness of potential perimenopausal influences. A previous contact with mental health services had led to a referral for attention-deficit/hyperactivity disorder (ADHD), which was not subsequently supported. During assessment, she noted that her most intense episodes of worry occurred in the late morning, typically following poor sleep, skipped breakfast, and increased caffeine and sugar intake.
Using a TED-informed framework, these episodes were reformulated as reflecting not only psychological stress but also fatigue and metabolic instability. Initial intervention focused on stabilising these domains: sleep training, reducing caffeine and sugar intake, improving nutritional adequacy (including micronutrient support where indicated), and introducing a consistent routine of exercise, relaxation, and recovery practices.
As physiological stability improved, the client was better able to engage in psychological work, including exploring beliefs related to menopause, health, and identity. Subsequent consultation with her GP led to the initiation of hormone replacement therapy (HRT), which further contributed to improvements in overall quality of life. What initially felt overwhelming became more manageable as the underlying regulatory load was reduced. This case illustrates how addressing physiological load may facilitate engagement with psychological processes during the perimenopausal transition
Common Negative Beliefs and Associated Behavioural Patterns
The menopausal transition is often accompanied by shifts in the interpretation of internal states and significant alterations to self-image. A long history of mental illness complicates the picture even more. The following belief–affect–behaviour patterns are commonly observed:
- “Something is wrong with me”
Affect: anxiety, confusion, hypervigilance
Behaviour: symptom checking, excessive reassurance seeking, or avoidance of medical consultation - “I’m losing control of my body and mind”
Affect: fear, helplessness
Behaviour: withdrawal from demands, reduced decision-making, disengagement from responsibilities - “I can’t cope like I used to. This is embarrassing; Sex is not the same. I will end up alone”
Affect: shame, frustration
Behaviour: avoidance of challenge, argumentative, over-reliance on others, reduced role engagement - “This is permanent and will only get worse”
Affect: hopelessness
Behaviour: reduced help-seeking, disengagement from treatment or behavioural change - “I’m becoming less capable”
Affect: self-doubt, embarrassment
Behaviour: avoidance of cognitively demanding or evaluative situations - “I’m not myself anymore”
Affect: identity disturbance, grief
Behaviour: social withdrawal, loss of engagement in valued activities - “Other people will notice and judge me”
Affect: social anxiety
Behaviour: avoidance of visibility (meetings, presentations, social interaction) - “Exercise will make things worse. I’m too exhausted”
Affect: fatigue, apprehension
Behaviour: inactivity, loss of routine, reduced exposure to beneficial physiological stress - “I just need to push through this”
Affect: internal pressure
Behaviour: paradoxical avoidance of rest and recovery, leading to further dysregulation - “I should be able to handle this on my own”
Affect: isolation, self-criticism
Behaviour: reduced help-seeking (medical, psychological, or social)
NA-CBT Formulation
From a NeuroAffective-CBT perspective, these patterns often emerge when physiological signals (raw affect) become fused with cognitive interpretation.
For example:
Physiological load →
Fatigue and hormonal fluctuation →
Increased limbic (amygdala) reactivity →
Threat-focused attention and cognitive interpretation (“I’m losing control”) →
Avoidance / compensatory / capitulatory behaviours →
Reduced regulatory capacity →
Increased instability →
Increased physiological load
This sequence operates as a self-reinforcing loop. Behavioural responses such as avoidance, overcompensation, or capitulation may reduce distress in the short term, but they contribute to the maintenance of the problem through several interacting mechanisms.
First, they reinforce threat perception and amplify raw affect. When internal states are repeatedly interpreted as dangerous or unmanageable, the nervous system becomes increasingly sensitised, heightening vigilance toward bodily sensations and emotional shifts.
Second, they reduce exposure to corrective experiences. Avoiding situations, sensations, or demands limits opportunities to learn that these internal states are tolerable, transient, and manageable. As a result, threat-based interpretations remain unchallenged.
Third, these behaviours constrain opportunities for physiological regulation. Reduced movement, disrupted routines, poor sleep, and inconsistent nutrition can increase physiological load, narrowing the system’s capacity to recover from activation.
Over time, these processes interact to maintain both physiological and psychological dysregulation. Increased instability feeds back into elevated physiological load, perpetuating the cycle and increasing the likelihood that future internal states will again be interpreted as threatening.
Intervention within this framework focuses on interrupting this loop by stabilising physiological load, modifying threat-based interpretation, and reintroducing corrective behavioural experience.
Clinical Implications
The therapeutic aim is not the immediate elimination of these beliefs, but the creation of conditions in which they can be re-evaluated more flexibly.
This involves:
- differentiating physiological state from interpretation
- stabilising underlying regulatory systems (TED: sleep, exercise, nutrition)
- gradually reintroducing avoided or restricted behaviours
As regulatory stability improves, interpretation becomes less rigid and more context-sensitive. This supports a shift from:
“Something is wrong with me”
to
“My system is under load, and can be supported”
Plain-Language Summary
Perimenopause is not just hormonal; it affects the whole system — brain, body, and behaviour.
Hormonal changes influence mood, sleep, stress sensitivity, and cognitive clarity. At the same time, the brain, immune system, and gut interact in ways that shape how these changes are experienced.
From a NeuroAffective-CBT perspective, these are not simply “symptoms”, but signals that the system is operating under increased regulatory load. By supporting sleep, movement, and nutrition, individuals can reduce this load and improve emotional regulation. These lifestyle interventions can then be complemented by targeted cognitive and behavioural strategies.
Rather than being only a period of disruption, perimenopause can also represent an opportunity to develop more stable and adaptive patterns of functioning, adjust expectations, and strengthen coping and self-efficacy in preparation for the next stage of transition.
Conclusion
Perimenopause can be understood as a period of multi-system adjustment involving endocrine, neural, immune, and metabolic processes. The variability in individual experience reflects the complexity of these interacting systems rather than a single causal pathway.
From a NeuroAffective-CBT perspective, this transition highlights the importance of integrating physiological regulation into psychological formulation. Changes in mood, cognition, and behaviour are not solely psychological in origin, but often reflect shifts in underlying regulatory systems operating under increased load.
This perspective has practical implications. Interventions that stabilise sleep, support nutritional adequacy, and maintain appropriate levels of physical activity may help reduce background physiological volatility, creating conditions in which emotional regulation and cognitive flexibility can be more effectively supported.
Within this framework, the aim is not to eliminate distress, but to improve the system’s capacity to move between states of activation and recovery with greater stability and predictability. As regulatory capacity improves, individuals are better able to differentiate between physiological signals and their interpretation, reducing the likelihood that transient internal states are experienced as overwhelming or self-defining.
In this way, perimenopause can be understood not only as a period of challenge, but also as an opportunity for recalibration. When supported appropriately, this transition may facilitate the development of more stable regulatory patterns across physiological and psychological domains, contributing to long-term resilience and adaptive functioning.
Perimenopause is not merely an endocrine event but a biopsychophysiological transition with implications for affect regulation, cognition, sleep, and behaviour. A NeuroAffective-CBT formulation may be clinically useful insofar as it integrates physiological state, emotional processing, and behavioural adaptation. Within this framework, interventions targeting sleep regularity, movement, nutrition, stress recovery, and cognitive appraisal may help reduce regulatory load and support more flexible functioning during the menopausal transition. However, the specific contribution of NA-CBT remains a clinical formulation model rather than an established evidence-based treatment protocol for perimenopausal distress.
Glossary of Key Terms
Perimenopause
The transitional phase before menopause, characterised by fluctuating levels of estrogen and progesterone, often accompanied by changes in mood, sleep, and physiological stability.
Menopause
The point at which menstruation has ceased for twelve consecutive months, marking the end of reproductive function.
Estrogen
A primary female sex hormone involved in reproductive function, but also influencing brain activity, mood regulation, bone health, and metabolic processes.
Serotonergic signalling
The activity of serotonin (a neurotransmitter) in the brain, involved in mood, emotional regulation, sleep, and cognition.
Synaptic plasticity
The brain’s ability to change and adapt by strengthening or weakening connections between neurons, supporting learning, memory, and emotional regulation.
Stress responsivity
The way the body and brain respond to stress, including activation of hormonal and nervous system pathways.
Gut–brain axis
The bidirectional communication system between the gastrointestinal tract and the brain, involving neural, immune, and metabolic pathways.
Estrobolome
The collection of gut bacteria capable of metabolising estrogen, influencing how estrogen is processed and recirculated in the body.
Short-chain fatty acids (SCFAs)
Metabolic by-products produced by gut bacteria that support immune function, gut integrity, and metabolic regulation.
Physiological load
The overall burden placed on the body’s regulatory systems, influenced by factors such as sleep, stress, nutrition, hormonal changes, and physical activity.
Raw affect
Immediate, pre-cognitive bodily signals of emotional or physiological states (e.g., tension, fatigue, heat, agitation).
Cognitive interpretation
The meaning or explanation the mind assigns to internal or external experiences (e.g., “something is wrong with me”).
Limbic (amygdala) reactivity
Increased activity in brain regions involved in threat detection and emotional processing, particularly the amygdala.
Threat-focused attention
A cognitive bias in which attention is directed toward perceived threats, including bodily sensations or emotional states.
Avoidance behaviours
Actions aimed at reducing distress by withdrawing from or avoiding perceived threats, often maintaining anxiety over time.
Compensatory behaviours
Actions intended to counteract or control perceived problems (e.g., overworking, excessive reassurance seeking), which may inadvertently maintain distress.
Capitulatory behaviours
Patterns of giving up or disengaging in response to perceived inability to cope, often associated with withdrawal or reduced functioning.
Regulatory capacity
The ability of the body and mind to return to a stable baseline following stress or activation.
Autonomic flexibility
The capacity of the nervous system to shift effectively between states of activation (stress) and recovery (rest).
Neuroplasticity
The brain’s ability to reorganise and adapt in response to experience, learning, and environmental demands.
NeuroAffective-CBT (NA-CBT)
An integrative cognitive-behavioural framework that incorporates physiological regulation (sleep, exercise, nutrition) into psychological formulation and intervention.
TED Framework (Tired–Exercise–Diet)
A model within NA-CBT focusing on three core regulatory domains: sleep/fatigue, physical activity, and nutrition.
Regulatory load
The cumulative demand placed on physiological and psychological systems, influencing emotional stability and cognitive function.
References
Anderson, D.J. (2016) Circuit modules linking internal states and social behaviour in flies and mice. Nature Reviews Neuroscience, 17(11), pp. 692–704.
Anderson, D.J. and Adolphs, R. (2014) A framework for studying emotions across species, Cell, 157(1), pp. 187–200.
Cortez, M. and Mirea, D. (2026) The transdiagnostic application of NeuroAffective-CBT: A case study of chronic stress and burnout. NeuroAffective-CBT®, London. Available at: ResearchGate.
Darwin, C. (1872) The expression of the emotions in man and animals. London: John Murray.
Dulcu, I. and Mirea, D. (2026) Treating panic disorder with vomiting-related safety behaviours using NeuroAffective-CBT: A case study of interoceptive threat and shame. NeuroAffective-CBT®, London. Available at: Academia.edu.
Gleeson, M., Bishop, N.C., Stensel, D.J., Lindley, M.R., Mastana, S.S. and Nimmo, M.A. (2011) ‘The anti-inflammatory effects of exercise: mechanisms and implications for the prevention and treatment of disease’, Nature Reviews Immunology, 11(9), pp. 607–615.
Mennitti, C. et al. (2024). How does physical activity modulate hormone responses? Biomolecules, 14(11), p. 1418.
Mirea, D. (2025) The use of lifestyle interventions in psychotherapy, NeuroAffective-CBT® [Online]. Available at: https://neuroaffectivecbt.com/2025/12/17/the-use-of-lifestyle-interventions-in-psychotherapy/ (Accessed: 14 April 2026).
National Institute for Health and Care Excellence (2024) Menopause: diagnosis and management (NG23). London: NICE. Available at: https://www.nice.org.uk/guidance/ng23 (Accessed: 15 April 2026).
Nieman, D.C. (2018) The compelling link between physical activity and the body’s defence system, British Journal of Sports Medicine, 52(13), pp. 789–790.
Popa, I. and Mirea, D. (2026) Physical Strength, Muscle Growth and Mental Health: Mechanisms linking resistance training to emotional regulation, neuroplasticity and immune function [Online]. Academia.edu. Available at: https://www.academia.edu/164833161/Physical_Strength_Muscle_Growth_and_Mental_Health_Mechanisms_linking_resistance_training_to_emotional_regulation_neuroplasticity_and_immune_function (Accessed: 14 April 2026)
Plottel, C.S. and Blaser, M.J. (2011) Microbiome and malignancy: the estrogen connection, Cell Host & Microbe, 10(4), pp. 324–335.
Strasser, B. (2015) ‘Role of physical activity and diet on mood, behaviour, and cognition’, Neuroscience & Biobehavioral Reviews, 57, pp. 107–123.
Related studies:
Pedersen, B.K. (2007) ‘Role of myokines in exercise and metabolism’, Journal of Applied Physiology, 103(3), pp. 1093–1098.
Peluso, M.A.M. and Guerra de Andrade, L.H.S. (2005) ‘Physical activity and mental health: the association between exercise and mood’, Clinics, 60(1), pp. 61–70.
Petersen, A.M.W. and Pedersen, B.K. (2005) ‘The anti-inflammatory effect of exercise’, Journal of Applied Physiology, 98(4), pp. 1154–1162.
Porges, S.W. (2011) The polyvagal theory: neurophysiological foundations of emotions, attachment, communication, and self-regulation. New York: W.W. Norton.
Ratey, J.J. and Loehr, J.E. (2011) ‘The positive impact of physical activity on cognition and brain function’, Journal of Applied Sport Psychology, 23(4), pp. 373–394.
Salmon, P. (2001) ‘Effects of physical exercise on anxiety, depression, and sensitivity to stress’, Clinical Psychology Review, 21(1), pp. 33–61.
Schuch, F.B., Vancampfort, D., Firth, J., Rosenbaum, S., Ward, P.B., Silva, E.S., Hallgren, M., Ponce De Leon, A., Dunn, A.L., Deslandes, A.C., Fleck, M.P. and Stubbs, B. (2018) ‘Physical activity and incident depression: a meta-analysis of prospective cohort studies’, American Journal of Psychiatry, 175(7), pp. 631–648.
Stonerock, G.L. et al. (2015) ‘Exercise as treatment for anxiety’, Annals of Behavioral Medicine, 49(4), pp. 542–556.
